Download presentation
Presentation is loading. Please wait.

1
CRRT (Continuous Renal Replacement therapy) Department of Nephrology Jeong Kyung Hwan
 Department of Nephrology Jeong Kyung Hwan")
2
Terminology Ultrafiltration fluid transport Diffusion Convection Solute transport Adsorption

3
Ultrafiltration Movement of fluid through a membrane caused by a pressure gradient (hydrostatic or osmotic pressure)
")
4
Diffusion Movement of solutes from an area of higher concentration to an area of lower concentration Dialysate is used to create a concentration gradient across a semi-permeable membrane the rate of diffusion is dependant on; – surface area of filter – ratio of dialysate flow to blood flow – size of the molecules

5
Convection Drag of solutes across a membrane during osmosis or ultrafiltration Used for removal of middle and large molecules Greater the amount of fluid that moves, the greater the solute loss

6
Diffusion vs. Convection

7
Terminology

8
Mechanism of Dialysis Ultrafiltration –Plasma water with solutes is drawn from the patient’s blood across the semipermeable membrane in the filter –The effluent pump controls the ultrafiltration rate automatically according to the set flow rates

9
Mechanism of Dialysis Haemofiltration –Plasma water with solutes is drawn from the patient’s blood across the semi-permeable membrane by means of ultrafiltration –A replacement solution is simultaneously infused into the blood flow path –Solute removal is achieved by convection (solvent drag across the membrane)
")
10
Replacement Fluids Pre - dilution Increase rate of filtration and convection Decrease rate of diffusion (concentration gradient) Decrease blood viscosity and therefore aids in extending the filter life Post – dilution Primarily replaces fluid and electrolyte losses No solute dilution Increased haemoconcentration Mechanism of Dialysis
 Decrease blood viscosity and therefore aids in extending the filter life Post – dilution Primarily replaces fluid and electrolyte losses No solute dilution Increased haemoconcentration Mechanism of Dialysis")
11
Haemodialysis –Unwanted solutes pass from the patient’s blood across the semi- permeable membrane and into the dialysate which is flowing in the opposite direction through the fluid compartment of the filter –Solute clearance is achieved by diffusion

12
Mechanism of Dialysis HaemoDiaFiltration –Haemodialysis and haemofiltration –Solute removal occurs by convection and diffusion –Fluid is removed by ultrafiltration. –Dialysate fluid is pumped through the fluid compartment of the filter. At the same time, the effluent pump controls the ultrafiltration rate –A replacement solution is infused into the blood flow path either before or after the filter – (pre or post dilution)
.")
13
Terminology CVVH –continuous venovenous hemofiltration CVVHD –continuous venovenous hemodialysis CVVHDF –continuous venovenous hemodiafiltration SCUF –slow continous ultrafiltration CAVHD –continuous arteriovenous hemodialysis

14
Classification of renal replacement therapies

15
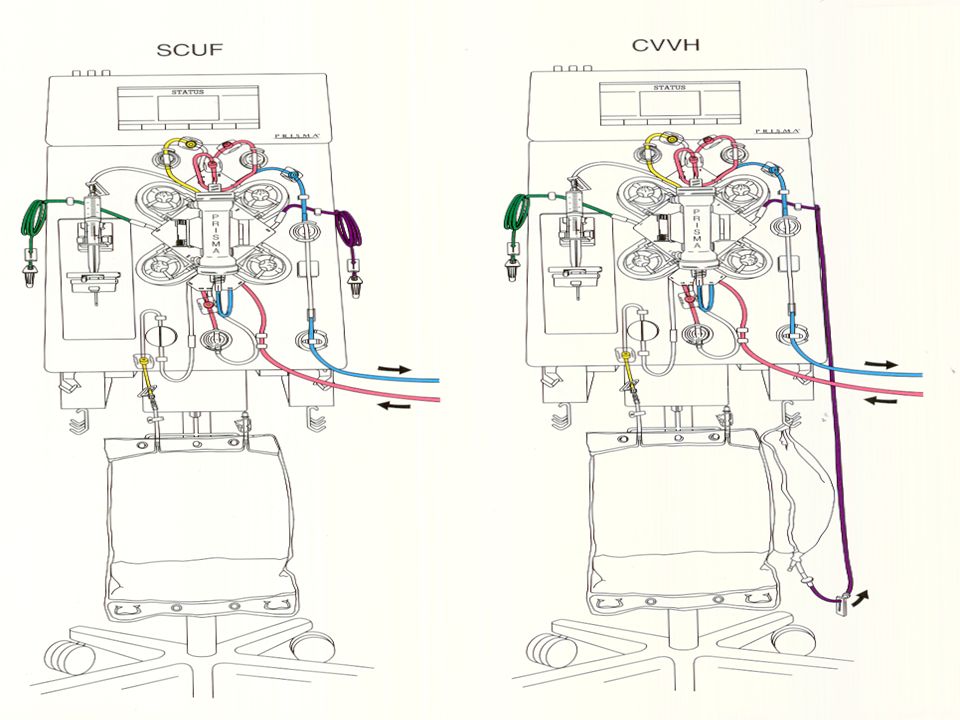
1) SCUF : Slow continuous UF Only fluid removal by Ultrafiltration (Maximum pt.fluid removal rate = 2000ml/hr) No dialysate fluid, No replacement fluid CRRT(Continuous Renal Replacement Therapy) 의 종류
 SCUF : Slow continuous UF Only fluid removal by Ultrafiltration (Maximum pt.fluid removal rate = 2000ml/hr) No dialysate fluid, No replacement fluid CRRT(Continuous Renal Replacement Therapy) 의 종류")
16
2) CAVH : continuous arterio-venous HF no blood pump: pt 의 동정맥압차에 의존 CRRT(Continuous Renal Replacement Therapy) 의 종류
 CAVH : continuous arterio-venous HF no blood pump: pt 의 동정맥압차에 의존 CRRT(Continuous Renal Replacement Therapy) 의 종류")
17
3) CVVH : Continuous veno-venous HF Solute removal by convection+ Safe fluid removal High clearance + Regulating UFR Substitution fluid : pre, post dilution Replacement solution flow rate = 100 to 4500ml/hr No dialysate fluid used
 CVVH : Continuous veno-venous HF Solute removal by convection+ Safe fluid removal High clearance + Regulating UFR Substitution fluid : pre, post dilution Replacement solution flow rate = 100 to 4500ml/hr No dialysate fluid used")
18
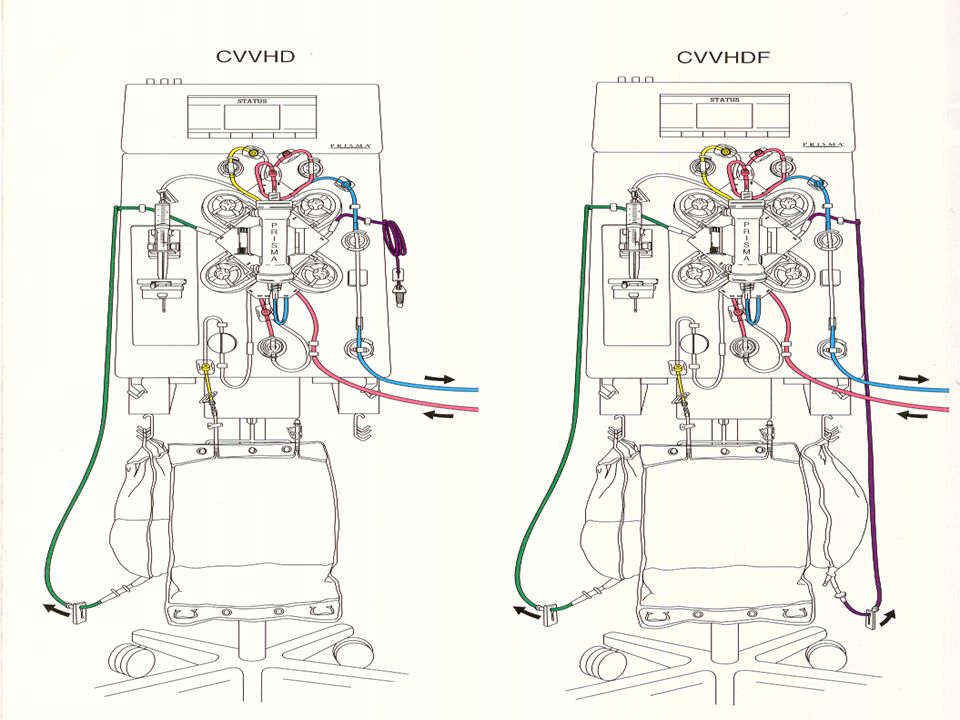
4) CVVHD : Continuous veno-venous HD Solute clearance by diffusion Urea clearance 가 CVVH 보다 높음 Azotemia 가 심한 환자 ( Dialysate – diffusion 기능 첨가 ) Dialysate solution flow rate = 50 to 2500ml/hr No replacement fluid
 CVVHD : Continuous veno-venous HD Solute clearance by diffusion Urea clearance 가 CVVH 보다 높음 Azotemia 가 심한 환자 ( Dialysate – diffusion 기능 첨가 ) Dialysate solution flow rate = 50 to 2500ml/hr No replacement fluid")
19
5) CVVHDF : Continuous veno-venous HDF Solute removal by Convection (HF) + Diffusion (HD) CRRT 중 가장 효과적인 치료방법 Replacement solution flow rate = 100 ~2000ml/hr Dialysate solution flow rate = 50 to 2500ml/hr
 CVVHDF : Continuous veno-venous HDF Solute removal by Convection (HF) + Diffusion (HD) CRRT 중 가장 효과적인 치료방법 Replacement solution flow rate = 100 ~2000ml/hr Dialysate solution flow rate = 50 to 2500ml/hr")
20
The PRISMA ® Communication Unit Flow Control Unit Fluid Control Unit

21
® Communication Unit

22
Status Screen CHANGE BAGS NORMALIZ BLOOD TREAT HISTORY HELP SET FLOW RATES SETUPSTANDBY RUN ENDSCUF CVVH CVVHDF CVVHD Communication Unit Touch-screen Current Flow Rates Blood Flow Rate: Replacement Rate : Dialysate Flow Rate: Anticoagulation: Treatment Data Time: Dialysis Fld used: Replacement Fld used Total Effluent: Actual fluid removed: Current Pressures Access: Filter Pres: Effluent: Return: TMP: ΔP: Next Intervention: 1 min Due to: Replacement bag empty MODIFY SETTINGS EXAMINE ALARMS

23
® Flow Control Unit

24
Blood Leak Detector Air Bubble Detector Return Line Clamp Flow Control Unit - Safety

25
® Fluid Control Unit

28
Dialysate(D) urea urea middle Modality Blood Replacement Clearance Clearance Molecular pump fluid(RF) (L/d) (ml/min) Clearance Simplicity SCUF Yes/No No 1-4 1-3 + + CAVH No RF 10-15 7-10 + + + CVVH Yes RF 22-24 15-17 + + + + + CAVHD No D 24-30 17-21 – + CVVHD Yes D 24-30 17-21 – + + CAVHDF No RF+D 36-38 25-26 + + + + + + CVVHDF Yes RF+D 36-38 25-26 + + + + + + Symbols: +, most simple ; + + +, most difficult Comparison of different CRRT modalities
 urea urea middle Modality Blood Replacement Clearance Clearance Molecular pump fluid(RF) (L/d) (ml/min) Clearance Simplicity SCUF Yes/No No CAVH No RF CVVH Yes RF CAVHD No D – + CVVHD Yes D – + + CAVHDF No RF+D CVVHDF Yes RF+D Symbols: +, most simple ; + + +, most difficult Comparison of different CRRT modalities")
29
CRRT -Hemodynamic status 가 불안정한 다장기부전 (multiple organ failure) 및 기타 여러 가지 합병증들이 동반된 급성 신부전의 치료방법 - 생체적합성과 투과성이 우수한 혈액여과막을 사용하며, 대류 (convection) 와 확산 (diffusion) 에 의해 용질의 제거가 이루어짐 - 혈액여과막의 수분투과성이 높아 혈역동의 큰 변화없이 다량의 수분 제거 가능 - 혈액여과막의 표면에 ß2-microglobulin, TNF, inflammatory mediators 등이 흡착되어 제거됨
 및 기타 여러 가지 합병증들이 동반된 급성 신부전의 치료방법 - 생체적합성과 투과성이 우수한 혈액여과막을 사용하며, 대류 (convection) 와 확산 (diffusion) 에 의해 용질의 제거가 이루어짐 - 혈액여과막의 수분투과성이 높아 혈역동의 큰 변화없이 다량의 수분 제거 가능 - 혈액여과막의 표면에 ß2-microglobulin, TNF, inflammatory mediators 등이 흡착되어 제거됨")
30
Differences between IHD and CRRT

31
CRRT Treatment Goals - Maintain fluid,electrolyte,acid/base balance - Prevent further damage to kidney tissue - Promote healing and renal recovery - Allow other supportive measures ; nutritional support

32
Application Diseases (Indication of CRRT) Renal indication a. ARF + Cardiology failure : 기존 HD 시 저혈압이 발생되어 신기능회복이 지연되는 환자의 경우, CRRT 는 혈액동력학적 안정성이 있어 부작용 없이 신기능 회복을 도울 수 있다. b. ARF + Cerebral Edema : 점차적이고 느린 삼투압의 감소로 투석 불균형증을 예방할 수 있다. c. ARF + Hypercatabolism : 비경구적 영양공급으로 안정되고 적절한 탈수조절이 가능하다.

33
Non-renal indication a. Sepsis & other inflammatory disease - 염증매개체를 체외 순환을 통해 감소시켜 증상을 호전 시킨다. - 염증매개체는 고분자량이므로 convection 과 high flux membrane 을 통해 감소 된다. b. ARDS ( acute respiratory disorder syndrome ) - 가스 교환과 심박출량 감소를 유도한다. c. Cardiopulmonary Bypass - CPB 동안 과도한 수분과 염증매개체를 제거한다. d. Crush Syndrome - 지속적인 HF 로 myoglobulin 의 배출을 증가시켜 ARF 를 예방한다. e. Lactic Acidosis - Bicarbonate 를 이용한 CRRT 로 산증을 교정할 수 있다. f. Congestive heart failure - 이뇨제나 혈관확장제에 반응이 없는 CHF 환자에게 과다한 수분제거가 가능하다. Application Diseases (Indication of CRRT)
 - 가스 교환과 심박출량 감소를 유도한다. c. Cardiopulmonary Bypass - CPB 동안 과도한 수분과 염증매개체를 제거한다. d. Crush Syndrome - 지속적인 HF 로 myoglobulin 의 배출을 증가시켜 ARF 를 예방한다. e. Lactic Acidosis - Bicarbonate 를 이용한 CRRT 로 산증을 교정할 수 있다. f. Congestive heart failure - 이뇨제나 혈관확장제에 반응이 없는 CHF 환자에게 과다한 수분제거가 가능하다. Application Diseases (Indication of CRRT).")
34
CRRT treatment summary Fluid manage - CHF - ARDS - Fluid resuscitation - nutritional support Inflammatory mediator modulation - SIRS: MODS, ARDS, sepsis etc Electrolyte, acid-base balance - SIRS, CHF - catabolic conditions Uremic/azotemia control - ARF - catabolism - nutritional support

35
IHD vs. CRRT in ICU-RCT Nature Review Nephrol 2006

36
IHD vs. CRRT in AKI: Meta-analysis JAMA 2008 Mortality

37
IHD vs. CRRT in AKI: Meta-analysis JAMA 2008 Dialysis Dependency

38
IHD vs. CRRT in AKI: volume control and MAP 24hr fluid balance Baseline and Intradialytic MAP AJKD 2004

39
CRRT 적용 요인들

40
Advantages of CRRT over IHD in critical illness Allows adequate volume of nutrition without compromising fluid balance Decreased vasopressor requirements during fluid removal Increased hemodynamic stability Optimizes fluid balance in lung injury Continuous control of fluid balance

41
Early vs. Late CRRT Nephrology Board review course 2011 BUN 60mg/dl UO 100ml/8hr BUN 76mg/dl ICU adm 2day

42
Dose of CRRT Not used urea clearance – influence nutritional input, tissue catabolism, premorbid nutritional status, liver function, extracellular volume expansion –no correlation with higher molecular weights Use of effluent flow rate –Sum of net fluid removal, dialysate and replacement flow rate in predilution CVVHDF mode Target dose : 30-35ml/kg/hr

43
Flow setting Blood flow rate ─ maximum 180ml/min, usually 100-150 ml/min Replacement fluid rate –non- catabolic patient 인 경우 1,000 ml/hr 로 시작 hypercatabolic state 인 경우 1,000- 1,500 ml/hr 로 시작 –sepsis, ARDS with MOF patient 경우 1,000- 1,500 ml/hr 로 시작하 여 maximum 2,000 ml/hr 까지 증가시킴 Dialysate flow rate –1,000 ml/hr 로 시작하여 hypercatabolic patient 인 경우에는 2,500 ml/hr 까지 올릴 수 있다. (BFR 의 1/5 – 1/10 유지 )
.")
44
Patient removal Prescribed weight loss: 3 kg in 24 hours3000 ml Prescribed hyperalimentation: 2000 ml in 24 hours+ 2000 ml Urine output: 500 ml in 24 hours- 500 ml Desired patient fluid removal in 24 hours4500 ml Patient Fluid Removal Rate to be entered in ml/hr190 ml Ex) Saline flushing 100cc q1hr 100 ml Patient Fluid Removal Rate to be entered in ml/hr 290 ml
 Saline flushing 100cc q1hr 100 ml Patient Fluid Removal Rate to be entered in ml/hr 290 ml")
Similar presentations



. 생명의 특징 (attributes of living matter) Six most important life processes Metabolism ( 신진대사 ) Responsiveness ( 반응, adaptation.>")






 BL4 방문협의>")

 비만률순위 : 29 위 (2005 OECD)>")


>")



