Download presentation
Presentation is loading. Please wait.

2
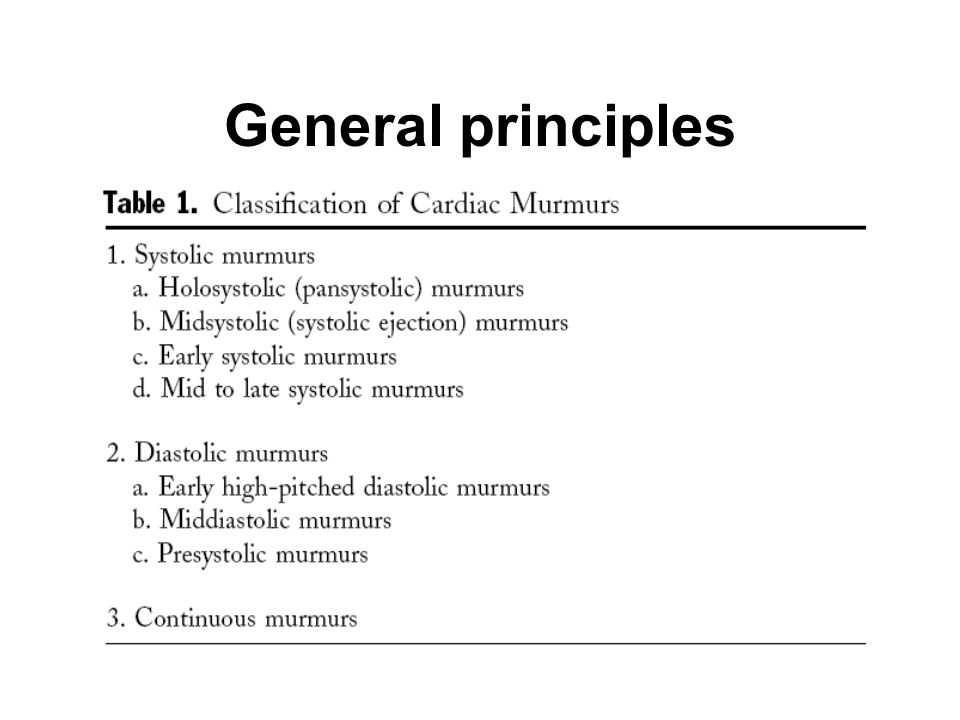
1.Introduction Cardiac ausculation remains the most widely used method of screening for VHD. -systolic m.: 대부분, 병적이 아님. -diastolic m. & continuous m : 거의 언제나 병적인 상태를 반영 General principles

6
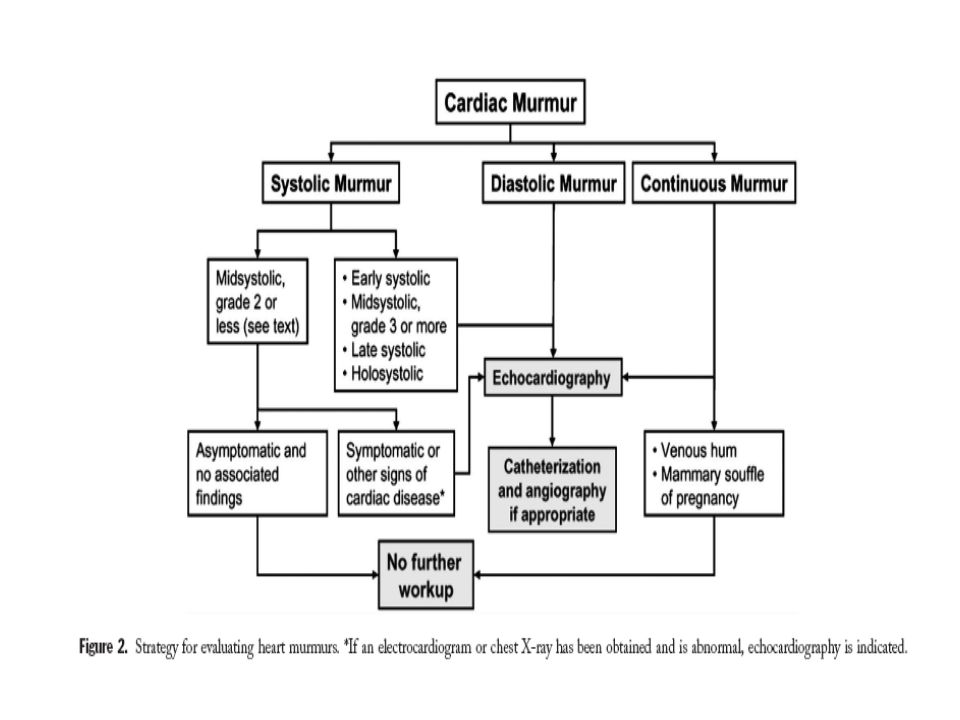
Venous hum: a continous musical murmur heard on ausculation over the major veins at the base of the neck. It is audible paticularly when the patient is anemic, upright, and looking to the contralateral side. It is also heard in some healthy, young individuals. Mammary souffle of pregnancy?

7
General principles Innocent murmur 의 특징들 > - Lt. Sternal border 에서 들리는 grade 1 or 2 의 m. - Systolic ejection pattern(midsystolic) - S2 의 정상적 강도와 분열 - 다른 이상 음이나 잡음이 없음 - 심비대나 확장의 소견이 없고, valsalva maneuver 나 쭈그리고 있다가 일어날 시 강도의 증가가 없음.
 - S2 의 정상적 강도와 분열 - 다른 이상 음이나 잡음이 없음 - 심비대나 확장의 소견이 없고, valsalva maneuver 나 쭈그리고 있다가 일어날 시 강도의 증가가 없음..")
8
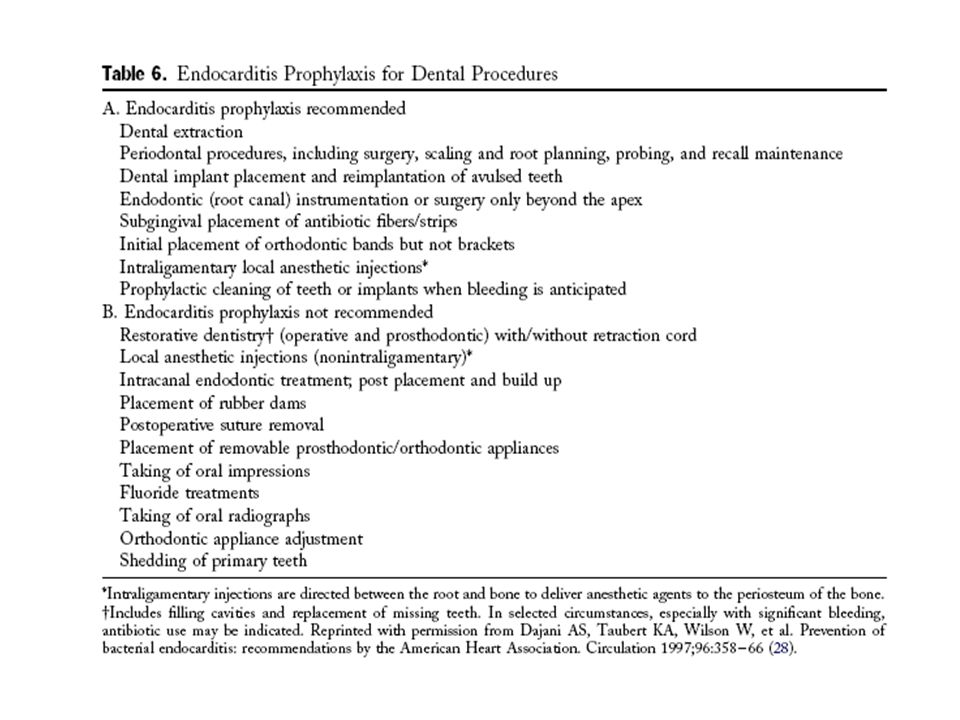
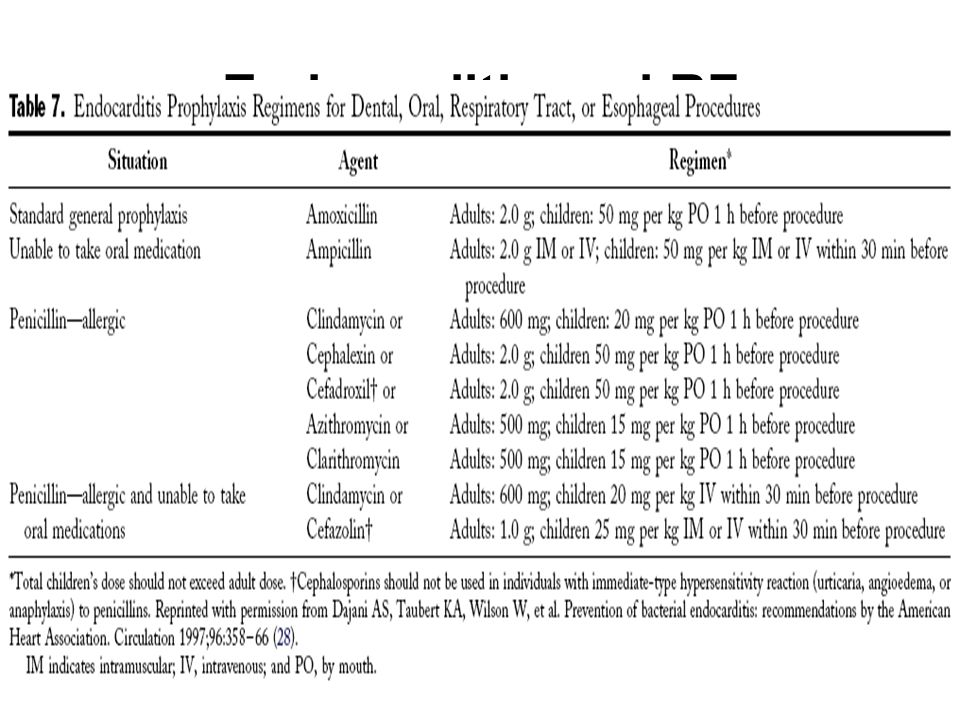
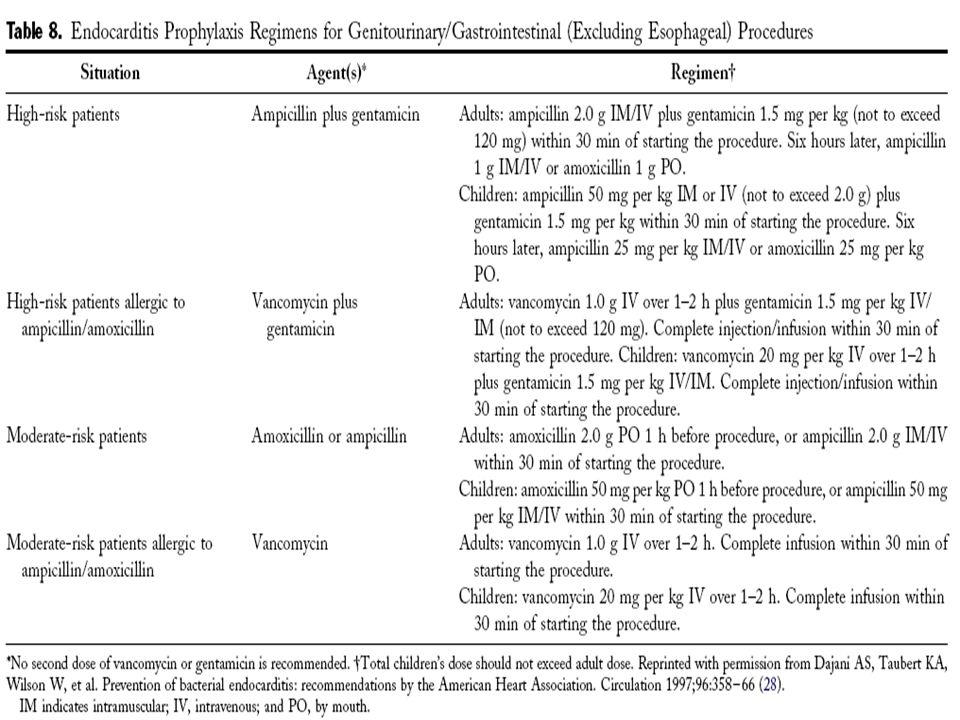
Endocarditis and RF Prophylaxis Infective endocariditis - 상당한 이환율과 사망률과 관련이 있는 중한 질 환. - 비정상적으로 빠른 혈류가 심내막에 손상, 잇다 른 thrombosis 와 vegetation 침착

9
Endocarditis and RF Prophylaxis Endocarditis prophylaxis Class I: Recommended -IE Hx.(+) + prosthetic heart valve -Complex cyanotic congenital heart dz.(e.g., single- ventricle states, transposition of the great arteries, tetralogy of Fallot) -Sugically constructed systemic pulmonary shunts or conduits. -Congenital cardiac valve malformations, particularly bicuspid aortic valve & acquired valvular dysfunction.(e.g. RHD) -Pt. Who have undergone valve repair -HCMP when there is latent or resting obstruction. -MVP+ 청진상 VR and/or Echo 상 thickened leaflets 이 있는 경 우
 -Pt. Who have undergone valve repair -HCMP when there is latent or resting obstruction. -MVP+ 청진상 VR and/or Echo 상 thickened leaflets 이 있는 경 우.")
10
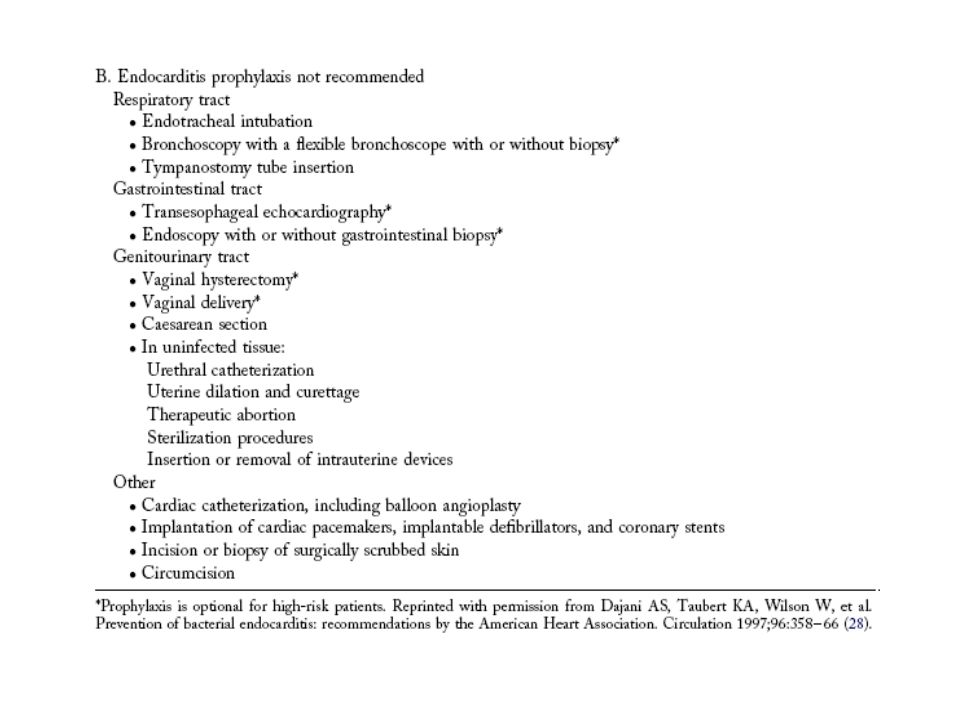
Endocarditis and RF Prophylaxis Class III: Not recommended -isolated secundum ASD -ASD, VSD, PDA 의 성공적인 수술적 혹은 경피적 교 정 후 6 개월이 지난 경우 -MVP s (MR or thickend leaflets by Echo) -Physiological, functional, or innocent m including Aortic valve sclerosis ( 정의상, Echo 상, increased echogenicity, thickening of leaflets s restriction of motion and a peak velocity less than 2.0 m/s) -murmur 가 없고, Echo 상, 정상 구조인, physiologic MR -murmur 가 없고, Echo 상, 정상 구조인, physiologic TR and/or PR
 -Physiological, functional, or innocent m including Aortic valve sclerosis ( 정의상, Echo 상, increased echogenicity, thickening of leaflets s restriction of motion and a peak velocity less than 2.0 m/s) -murmur 가 없고, Echo 상, 정상 구조인, physiologic MR -murmur 가 없고, Echo 상, 정상 구조인, physiologic TR and/or PR")
11
Endocarditis and RF Prophylaxis

16
Rheumatic fever prophylaxis -VHD 의 중요한 원인

17
Endocarditis and RF Prophylaxis Rheumatic fever prophylaxis -VHD 의 중요한 원인

18
Endocarditis and RF Prophylaxis Rheumatic fever prophylaxis -VHD 의 중요한 원인

19
Aortic stenosis 1. 원인 - 가장 흔한 원인은 normal AV 의 calcification(AS 와 유사한 작용 ) 혹은, congenital bicuspid valve. - 덜 흔한 원인은 Rheumatic AS
 혹은, congenital bicuspid valve. - 덜 흔한 원인은 Rheumatic AS.")
20
Aortic stenosis 2.Grading

21
Aortic stenosis 3.Pathophysiology AS -> Continuous pressure load -> LVH 초기 : 증가된 LV wall thickness 가 압력차를 이기는 동시에, LV systolic wall stress(afterload) 도 정상 범위로 유지 ; EF, 정상범위로 유지됨 -> LVH 의 진행 ① wall stress 가 증가되고, 심근수축력 감소로 EF 감소하기 시작
 도 정상 범위로 유지 ; EF, 정상범위로 유지됨 -> LVH 의 진행 ① wall stress 가 증가되고, 심근수축력 감소로 EF 감소하기 시작")
22
Aortic stenosis 3.Pathophysiology AS -> Continuous pressure load -> LVH 초기 : 증가된 LV wall thickness 가 압력차를 이기는 동시에, LV systolic wall stress(afterload) 도 정상 범위로 유지 ;EF, 정상범위로 유지됨 -> LVH 의 진행 ① wall stress 가 증가되고, 심근수축력 감소로 EF 감소하기 시작
 도 정상 범위로 유지 ;EF, 정상범위로 유지됨 -> LVH 의 진행 ① wall stress 가 증가되고, 심근수축력 감소로 EF 감소하기 시작")
23
Aortic stenosis -> LVH 의 진행 ② low volume/mass ratio & compliance 감소 -> LVEDP ↑ -> LA contraction ↑ -> AF 발생 -> LVH 의 진행 ③ coronary blood flow/g of muscle 의 감소 -> ischemia ↑

24
Aortic stenosis 4.Natural History ① Latent period: 장기간의 무증상기 ② Moderate stenosis 에 도달하면 악화 진행 jet v. 0.3 m/s/y mean pr. Gr. 7 mm Hg/y ↑ valve area 0.1m 2 /y↓ -> 모든 무증상 mild-moderate AS 환자에 게 정기적인 F/U 을 요한다.

25
Aortic stenosis ⑤ ” Aortic sclerosis ” : - ventricular outflow 의 줄어듬없이, valve 의 thickening 이 있는 상태. - 65 세 이상의 25% 에서 발견됨 - AS 로의 진행, MI 와 Cardiovascular death 로의 위험성 50% 증가됨.

26
Aortic stenosis ⑥ Severe AS 에서 혈소판기능감소와 vW factor 수의 감소가 입증됨 -> bleeding ↑ -> AS 의 severity 와 관련이 있으며 MVR 후에는 정상으로 회복됨

27
Aortic stenosis ⑦ Sx.(angina,syncope,HF) 의 Onset - 한 번 증상이 발현하면 평균 수명 2-3yr - 그러므로 증상의 발현은 AS 경과의 중요한 전환점이 된다. - 증상 발현시부터, 수술이 일반적으로 추천된다. ⑧ Sudden death - 주로 증상있는 환자에게서 일어난다.

28
Aortic stenosis 5. 무증상 AS 의 Management - 증상이 없을 시에는 예후는 같은 연령 대의 정상인과 동일. - 증상 혹은 event 의 발현은 AS 의 severity 에 비례.

29
Aortic stenosis 5.1. AS 의 Classic findings L oud(grade4/6), late-peaking systolic murmur that radiates to the carotids, A single or pradoxically split S2, Delayed and diminished carotid upstroke - > confirm the severe AS -> Echo 를 해야
, late-peaking systolic murmur that radiates to the carotids, A single or pradoxically split S2, Delayed and diminished carotid upstroke - > confirm the severe AS -> Echo 를 해야.")
30
Aortic stenosis 6. Surgery -AVR(Replacement) -Aortic Balloon Valvotomy(ABV) -AVR 이 choice -ABV 를 할 수 있는 경우 비교적 젊은 Congenital or rheumatic AS
 -Aortic Balloon Valvotomy(ABV) -AVR 이 choice -ABV 를 할 수 있는 경우 비교적 젊은 Congenital or rheumatic AS.")
31
Aortic stenosis 5.Management

32
Aortic Regurgitation 1. 원인 흔한 원인들 : Idiopathic dilatation of the aorta, congenital abnormalities, calcific degeneration, rheumatic dz., IE, HTN, Myxomatous degeneration,dissection of ascending aorta, Marfan syndrome.

33
Aortic Regurgitation 1.1. Severity

34
Aortic Regurgitation 2.Acute AR 2.1. 병생리 IE,AD,Trauma -> volume overload -> LAP & LVEDP ↑↑ -> CO↓ -> pul. Edema and cardiogenic shock -> subendocardium 의 관류압감소와 LV wall 의 확장과 얇아지면서 후부하의 증가, 결과적으로 심근산소요구량 증가 -> ischemia 유발

35
Aortic Regurgitation 2.2. 진단 chronic AR 과 달리 특징적인 소견이 없다. 2D Echo : “ rapid pressure equilibrium ” AD 이 의심될 시 TEE 가 Ix. 이 된다. CT or MRI aortography,catheterization,CAG 등은 특별 한 경우 아니면 잘 안 한다.

36
Aortic Regurgitation 2.3. 치료 폐부종, 심실부정맥, electromechanical dissociation, collapse 등으로 사망이 흔하여, Urgent surgery 가 추 천된다. 술전에 Nitroprusside(LVEDP 감소 ), Inotropics 등이 도움이 될 수 있다. IABP 는 CIx. b-blocker 는 주의하여 사용 : reflux tachycardia 를 억제 IE 로 인한 AR 의 경우 surgery 를 늦추어야 한다.
, Inotropics 등이 도움이 될 수 있다. IABP 는 CIx. b-blocker 는 주의하여 사용 : reflux tachycardia 를 억제 IE 로 인한 AR 의 경우 surgery 를 늦추어야 한다..")
37
Aortic Regurgitation 3.Chronic AR 3.1. 병생리 AR-> LVD & LVH -> decompensated phase

38
Aortic Regurgitation 3.2.Natural history 1)Asymptomatic pts c normal LV function 9 studies; 증상발현 혹은 LV systolic dysfunction 으로의 진행률은 평균 4.3 %/y 평균 사망률 0.2 %/y ¼ 이상이 증상발현전 사망하거나 systolic dysfunction 이 된 다. Risk factors: age, LVES dimension, LVEDV, EF during exercise

39
Aortic Regurgitation 2) Asymptomatic pts c depressed LV function 증상발현으로의 진행률은 평균 25 ↑ %/y 대부분, 2-3 년내에 증상을 나타냄. 3) Symptomatic pts angina->mortality of 10 ↑ % /y HF-> mortality of 20 ↑ % /y
 Symptomatic pts angina->mortality of 10 ↑ % /y HF-> mortality of 20 ↑ % /y.")
40
Aortic Regurgitation 3.3. Diagnosis & Initial evaluation 1) Physical findings - diastolic m, displaced LV impulse, wide PP, - charcteristic peripheral findigs that reflect wide PP - S3 -Austin-Flint rumble (specific findings for sever AR); a low-pitched sound. It is typically heard during ventricular middiastole at the apex.
 Physical findings - diastolic m, displaced LV impulse, wide PP, - charcteristic peripheral findigs that reflect wide PP - S3 -Austin-Flint rumble (specific findings for sever AR); a low-pitched sound. It is typically heard during ventricular middiastole at the apex..")
41
Aortic Regurgitation 3.4. Medical Therapy Vasodilater: SV↑, AR↓-> LVEDV, wall stress,afterload ↓ -> EF↑, LVH↓ Nitroprusside, hydralazine iv, CCB,ACEI

42
Aortic Regurgitation Class I : chronic and severe AR + (Sx (+) or LVd (+)) & inoperable -> vasodilater Class IIa: Severe HF Sx.(+) or LVd (+) 인 경우 op 전에 단기요법으로. Class IIb: Severe AR + Sx.(-) + LV dilatation (+) + LVd (-) -> 장기요법
 + LV dilatation (+) + LVd (-) -> 장기요법.")
43
Aortic Regurgitation Class III Sx.(-) + mild to moderate AR + LVd (-) Sx.(-) + LVd(+) ; op 후보자 SX.(+) + (LVd(-) or mild to mod. LVd(+)) -> Long-term vasodilater 는 추천되지 않는다.
) -> Long-term vasodilater 는 추천되지 않는다..")
44
Aortic Regurgitation 3.5. Indication for AV Replacement or Repair - 대부분은 AV Replacement 를 한다. -replecement or repair 에 대한 적응증 은 다르지 않다. - 단, AV repair 를 시행하려면, 숙련된 operater, 충분한 경험을 가지고 있고, replacement 와 동 일한 성적을 입증한 center 에서 시행해야 한다.

45
Aortic Regurgitation

46
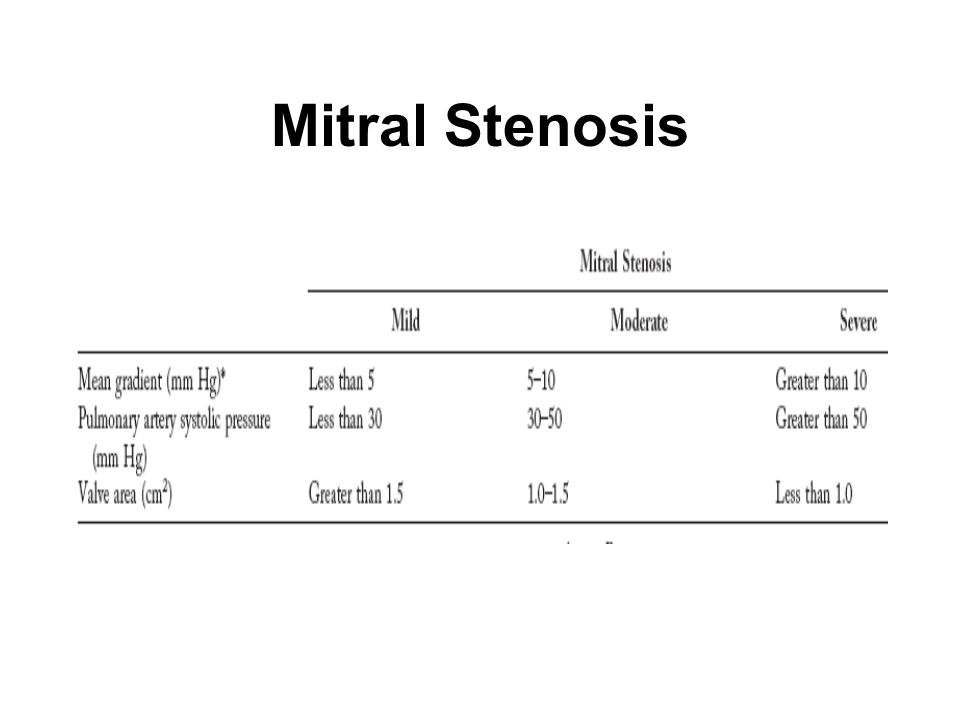
Mitral Stenosis 1.Pathophysiology and Natural Hx. 주원인은 Rheumatic carditis F:M 2:1 MS -> LAP↑ -> Pul. HTN RF 로 부터 증상 발현까지, 20-40yrs 증상발현 후 치료 안 할 시 10 YSR, 50-60% Significant limiting Sx.(+) ->10 YSR, 0-15% Severe pul. HTN ->3 년이내 사망 치료 안 한 MS 환자의 사망원인, 60-70%, pul. & sys. congestion. Systemic embolism 20-30%, pul. Embolism 10%, infection 1-5%
 ->10 YSR, 0-15% Severe pul. HTN ->3 년이내 사망 치료 안 한 MS 환자의 사망원인, 60-70%, pul. & sys. congestion. Systemic embolism 20-30%, pul. Embolism 10%, infection 1-5%.")
47
Mitral Stenosis 2.Diagnosis - C/M : fatigue,dyspnea, pul. Edema; AF,embolism ; hemoptysis, hoarseness, dysphagia -P/E : S1↑, OS, Low-pitched middiastolic rumble, presystolic m. *Severe AS: shorter A2-OS interval, longer duration of diastolic rumble, pul. HTN 의 findings (loud P2, RV heave) -2D Echo
 -2D Echo.")
48
Mitral Stenosis

50
3.Medical Therapy 3.1.General -RF & IE 에 대한 예방 - 운동제한, b-blocker, CCB -pul. Congestion 시, diuretics, salt restriction

51
Mitral Stenosis 3.Medical Therapy 3.2.AF - 증상있는 MS 환자의 30-40%.

52
Mitral Stenosis 3.Medical Therapy 3.3.Prevention of Systemic Embolization Class I: MS+ (AF or Prior emblic Hx. or LA thrombus) -> Anticoagulation is indicated. Class IIb: Severe MS + Sx(-) + LA ≥ 55mm Severe MS + LAE + spontaneous contrast -> Anticoagulation may be considered
 -> Anticoagulation is indicated. Class IIb: Severe MS + Sx(-) + LA ≥ 55mm Severe MS + LAE + spontaneous contrast -> Anticoagulation may be considered.")
53
Mitral Stenosis 3.Medical Therapy 3.4.Regarding Physical Activity and Exercise Severe MS 환자의 경우에서, 운동이 갑작스런 pul.venous pressure 를 높임으로써, pul. Edema 를 유발할 수 있다. -> Sx. Limited exercise. Low-level aerobic exercise

54
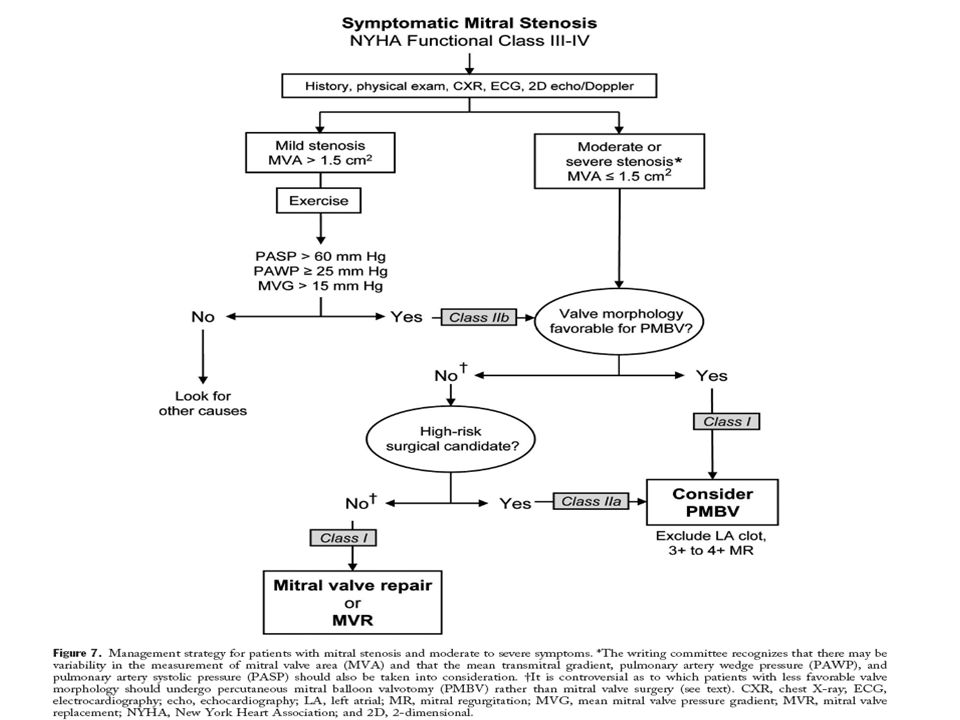
Mitral Stenosis 4.Evaluation of the Symptomatic Pt.

55
Mitral Stenosis

57
Mitral Valve Prolapse 1.Pathphysiology and Natural Hx. 정의 : 한 개 혹은 2 개의 mitral leaflets 이 LA 로 systolic billowing 하는 것. MR 이 동반될 수도 있음. Echo criteria: long-axis parasternal 혹은 다른 view 에서 mitral annulus 2mm 이상 위로 valve prolapse 가 있음. 대부분은 예후가 좋다. 나쁜 예후 : 동반된 MR 이 심할 수록, EF < 0.5, Thickend MV leaflets(≥5mm)
.")
58
Mitral Valve Prolapse 2.Evaluation and Management of the Asymptomatic Pt. Midsystolic click, a high-pitched soud of short duration. Normal lifestyle and regular exercise. IE prophylaxis is recommended for most pts, esp. who have MR(+),
,.")
59
Mitral Valve Prolapse 3.Evaluation and Management of the Symptomatic Pt. Class I: - TIA 있는 환자에게 -> Aspirin 75-325 mg/d - AF + (65 세 이상 혹은 HTN, MR murmur, HF) -> warfarin - -> aspirin - Stroke Hx.(+) + (MR, AF, LA thrombus) -> warfarin
 -> warfarin - -> aspirin - Stroke Hx.(+) + (MR, AF, LA thrombus) -> warfarin.")
60
Mitral Valve Prolapse Class IIa: - Stoke Hx.(+) s (MR,AF,LA thrombus), but, valve leaflets 의 thickening (≥ 5mm) and/or redunduncy -> warfarin. - Stroke Hx.(+) s (MR,AF,LA thrombus, valve thickening and/or redunduncy) -> aspirin - Aspirin 치료에도 불구하고 TIA 있는 경우 -> warfarin - Stroke Hx.(+), but CIx. TO antocoagulant -> aspirin Class IIb: - sinus rhyrhm 이지만 high risk 인 경우 -> aspirin
 s (MR,AF,LA thrombus, valve thickening and/or redunduncy) -> aspirin - Aspirin 치료에도 불구하고 TIA 있는 경우 -> warfarin - Stroke Hx.(+), but CIx. TO antocoagulant -> aspirin Class IIb: - sinus rhyrhm 이지만 high risk 인 경우 -> aspirin.")
61
Mitral Valve Prolapse 4.Surgery -flail mitral leaflet d/t rupture of chordae tendineae or their marked elongation -> op 를 고려해야 -ant. Leafleat MV repair 가 재수술률이 높다. - 수술을 고려해야할 인자들로서, HF Sx.,MR 의 severity, LV systolic function, LVED & ESV, pul. arterial pressure 등이 있다.

62
Mitral Regurgitation 1.Etiology 흔한 원인들 : MVP, RHD, CAD, IE, certain drugs, collagen vascular dz. LV dilatation 으로 인한 2 차적 원인으로.

63
Mitral Regurgitation 2.Acute Severe MR 2.1. Pathophysiology Avute severe MR -> Volume overload In LA & LV -> In the absence of compensatory eccentric hypertophy -> v wave ↑ & pul. congestion -> CO↓

64
Mitral Regurgitation 2.2.Diagnosis - S3 혹은 early diastolic rumble 가 유일한 finding 일 수 있다. - TTE 상, acute HF 와 hyperdynamic systolic function 이 동반시 severe MR 을 의심해봐야 한다. - 불확실할 시 TEE - CAD 동반시 CAG

65
Mitral Regurgitation

66
Mitral Regurgitation 2.3. Medical Therapy 제한된 역할, 주로 수술 전 혈역동학적으로 안정화 시키는 역할. 목적은 MR 과 pul. congestion 을 줄이고 SV 을 증가시키는 것. 혈압이 정상시 ->Nitroprruside iv 저혈압시 -> + inotropics OR -> aortic balloon couterpulsation 이 유용할 수 있다. IE 동반시 -> culture 와 antibiotics. 궁극적 치료는 surgery (MVr or MVR)
.")
67
Mitral Regurgitation 3.Chronic Asymptomatic MR 3.1.Pathophysiology and Natural Hx. MR 이 mild to moderate 시 혈동역학적 이상은 거의 나 타나지 않는다. MR sever 시 -> eccentric LVH, compensated phase -> decompensated phase; contractile function ↓: 진행하기 전에 MR 을 교정해 주어야 한다.

68
Mitral Regurgitation Severe MR 의 6-10 년내에 증상 혹은 LV dysfunction 이 생긴다. Natural history (d/t flail posterior leaflet) -10 년째, 90% 가 죽거나 op 를 요함. - 사망률 : 6-7% / y - 사망률 높은 군은, EF<0.6 or NYHA class III or IV -Sever Sx. 은 MVR 후에도 예후가 안 좋다.
 -10 년째, 90% 가 죽거나 op 를 요함. - 사망률 : 6-7% / y - 사망률 높은 군은, EF<0.6 or NYHA class III or IV -Sever Sx. 은 MVR 후에도 예후가 안 좋다..")
69
Mitral Regurgitation 3.2.Diagnosis Baseline exercise tolerance 를 정확히 평가하는 것이 중요하다. Displacement of the LV apical impulse-> severe and chronic MR 과 함께 cardiac enlargement 가 생겼음을 시사함 S3 or early diastolic rumble -> 반드시 LV dysfunction 을 의미 하는 것은 아니다. Pul. HTN 을 시사하는 소견은 advanced & poorer prognosis 를 의미.

70
Mitral Regurgitation 3.3.Medical Therapy 무증상이고 EF 이 정상인 경우 일반적으로 받아들여진 약물치료는 없다. Functional (d/t DCM) or ischemic MR 의 경우 preload 를 감소시키는 것이 reasonable 하다고 믿어 지고 있음. -LV systolic dysfunction 이 있는 경우 ; ACEI or b-blocker( 특히 CVD) and bibentricular pacing 이 MR 을 감소시키는 효과가 있음을 보여 주 었다.
 or ischemic MR 의 경우 preload 를 감소시키는 것이 reasonable 하다고 믿어 지고 있음. -LV systolic dysfunction 이 있는 경우 ; ACEI or b-blocker( 특히 CVD) and bibentricular pacing 이 MR 을 감소시키는 효과가 있음을 보여 주 었다..")
71
Mitral Regurgitation 3.3.Medical Therapy 증상이 있고, EF 은 정상인 경우, 수술이 가장 좋은 치 료이다. AF 동반시 ; -CCB,b blocker, digoxin, 드물게 amiodarone 등을 쓴다. -Op 시, Maze procedure 를 쓸 수도 있다. -INR 을 2.0-3.0 으로 유지하기.

72
Mitral Regurgitation 3.4.Indication for Surgery 3.4.1. Type of surgery -MVr(repair): 대부분의 경우 choice. MVR 에 비해 더 좋은 예후. valve 가 repair 에 적절해야하고, 숙련된 수 술의가 있어야한다. -MVR(replacement) c preservation of part or all of the mitral apparatus. -MVR c removal of mitral apparatus 예후가 가장 안 좋다.
: 대부분의 경우 choice. MVR 에 비해 더 좋은 예후. valve 가 repair 에 적절해야하고, 숙련된 수 술의가 있어야한다. -MVR(replacement) c preservation of part or all of the mitral apparatus. -MVR c removal of mitral apparatus 예후가 가장 안 좋다..")
73
Mitral Regurgitation

74
Tricuspid Valve Disease 1.Pathophysiology TV 의 이상은 거의 언제나 TR 로 된다. -RV systolic HTN: MS, PS, Pul. HTN -RV diastolic HTN: DCMP, RVI, RVF, -Pacemaker-induced severe TR -TV 자체의 이상 : Rheumatic valvulitis, IE, Carcinoid, RA, RT, Trauma, Marfan syn. TVP, TV annular dialatation, congenital dz., anorectic drugs.

75
Tricuspid Valve Disease 1.Pathophysiology TS, m/c, rheumatic origin.

76
Tricuspid Valve Disease 2.Diagnosis TS 의 임상상 : JVP 상 큰 a 파, y 파의 기울기 감소, OS, 흡기시 감소하는 presystolic or Middiastolic m., 다른 RVD 동반 ; MV and/or AV

77
Tricuspid Valve Disease 2.Diagnosis TR 의 임상상 : JVP 상 비정상적인 c 와 v 파 lower Lt. Parasternal systolic m ( 흡기시 증가 ; Carcallo ’ s sign) Middiastolic m. in severe TR, systolic hepatic pulsation, Dx. 은 2D Echo 와 Doppler echo
 Middiastolic m. in severe TR, systolic hepatic pulsation, Dx. 은 2D Echo 와 Doppler echo.")
78
Tricuspid Valve Disease 2.Diagnosis TS 의 임상상 :

79
Tricuspid Valve Disease 3.Management Class I: Severe TR + MVD -> MV surgery 시 TV repair 는 beneficial Class IIa : 1.Severe primary TR + Sx.(+) -> TVR or annuloplasty; reasonable 2.Severe secondary TR 이 annuloplasty 나 repair 로 교정할 수 없을 때, TVR 이 reasonable
 -> TVR or annuloplasty; reasonable 2.Severe secondary TR 이 annuloplasty 나 repair 로 교정할 수 없을 때, TVR 이 reasonable")
80
Tricuspid Valve Disease 3.Management Class IIb : Not severe TR 이면서 pul HTN 이나 TV annular dilatation 이 있는 경우, MV surgery 시 TV annuloplasty 를 고려해 볼 수 있다.

81
Tricuspid Valve Disease 3.Management Class III : 1.Sx (-) TR, PASP<60mmHg, normal MV 2.mild primary TR -> Not indicated of TVR or annuloplasty
 TR, PASP<60mmHg, normal MV 2.mild primary TR -> Not indicated of TVR or annuloplasty")
Similar presentations