Download presentation
Presentation is loading. Please wait.

1
수분과 소디움 순천향대학교 부천병원 신장내과 최 수정

2
Issues 체액과 전해질 Osmolarity 수분 balance Sodium balance Hypovolemia Fluid
Hyponatrmia & hypernatremia Potassium Balance Hypokalemia & hyperkalemia

3
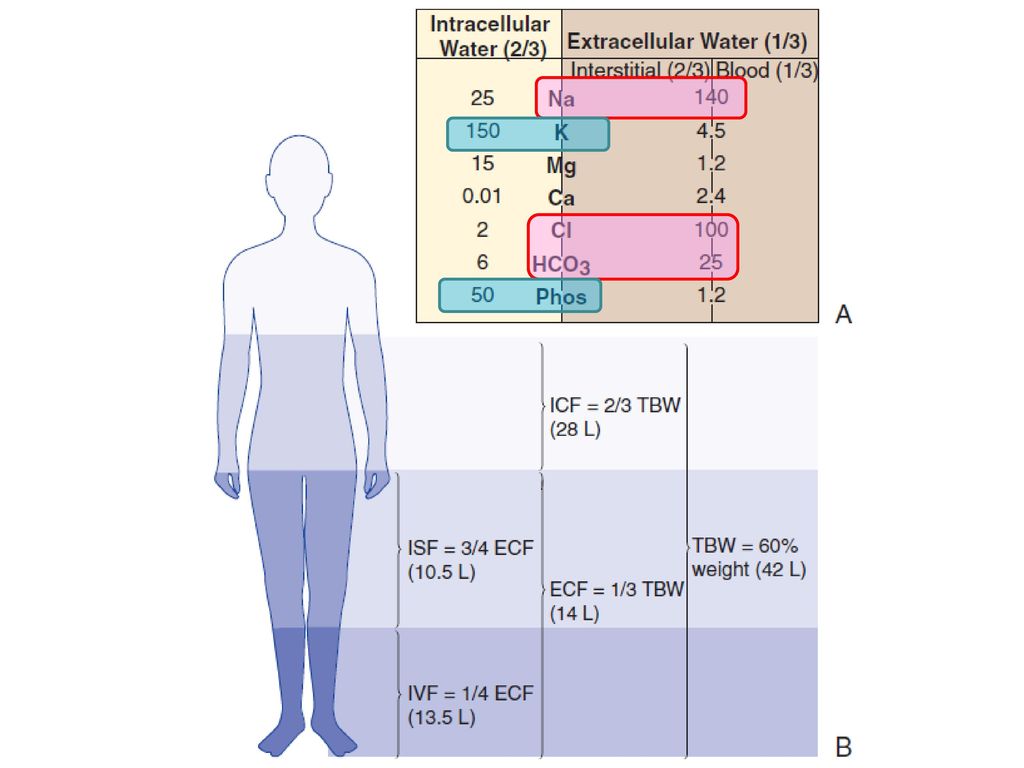
체액의 분포 총 체액량 (total body water): 남자 성인의 체중의 60%, 여자 성인, 비만 환자는 50%,
신생아나 유아는 70~80%

4
Stay hungry! Stay foolish!
70Kg 남자 ECF volume?

6
삼투질농도(osmolarity) 수액 내 용질의 농도,
물 kg당 milliosmole (mOsm/kg, mosmol/kg)로 표현 정상인 혈장 삼투질농도: 280 ~ 295mosmol/kg 혈장 삼투질 농도 (pOsm) = 2Na+(mEq/L) + glucose(mg/dL)/18 + BUN (mg/dL)/2.8 Tonicity: 수액이 이동하는 effective solute의 농도 Ineffective osmoles : urea
로 표현. 정상인 혈장 삼투질농도: 280 ~ 295mosmol/kg. 혈장 삼투질 농도 (pOsm) = 2Na+(mEq/L) + glucose(mg/dL)/18 + BUN (mg/dL)/2.8. Tonicity: 수액이 이동하는 effective solute의 농도. Ineffective osmoles : urea.")
7
체액의 분포 삼투질농도의 항상성 (ECF osmolarity= ICF osmolarity)은 세포막의 물의 자유로운 통과에 의한다.
은 세포막의 물의 자유로운 통과에 의한다.")
9
Water balance 배출 유입 Insensible Oral Gatrointestinal Enteral
parenteral 배출 Insensible Gatrointestinal Perspiratory renal

10
50/F CASE 1

11
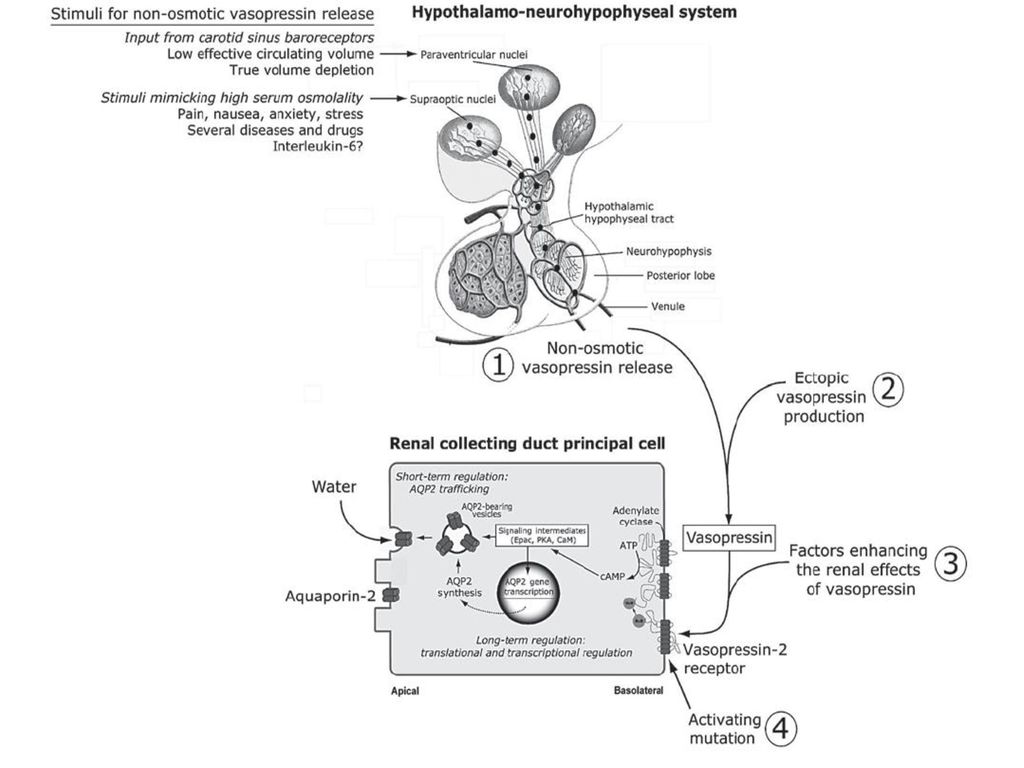
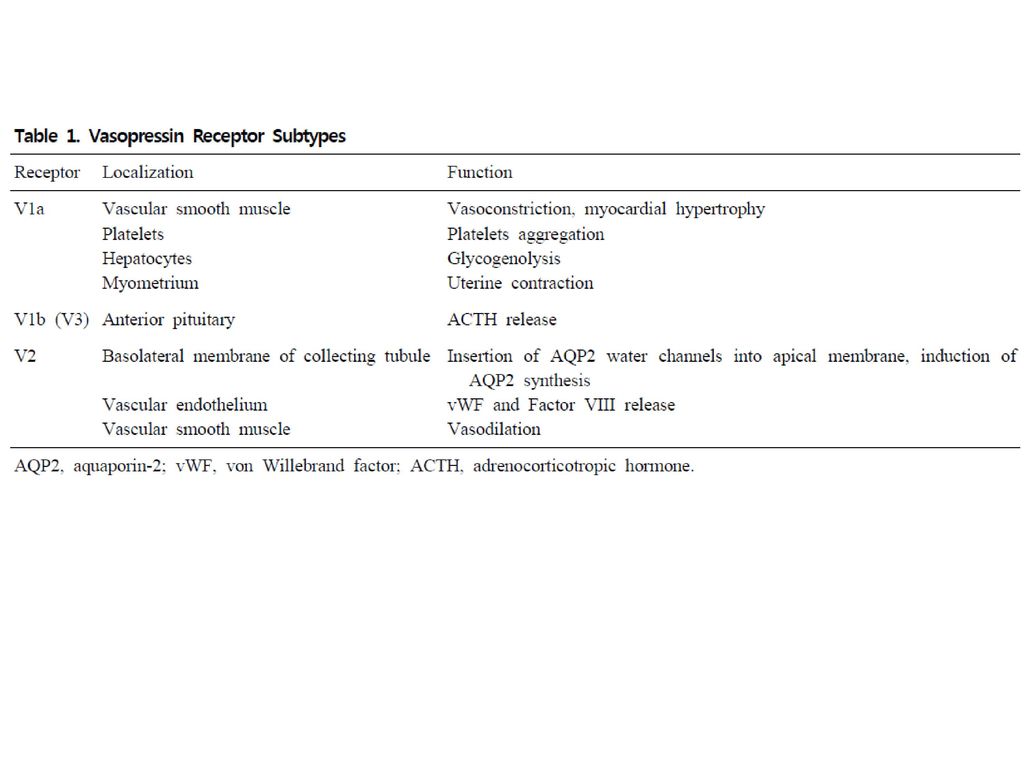
Water balance Osmo-regularion : hypotalamus Vasopressin secretion
Water ingestion: thirst Renal water excretion

14
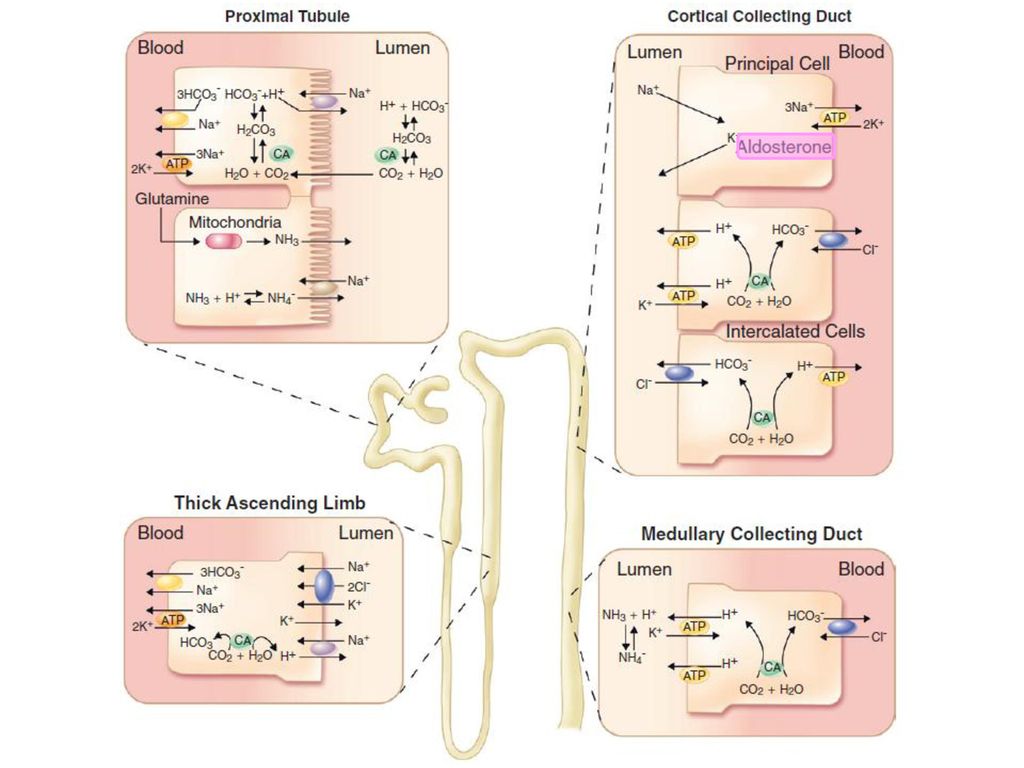
The renal concentrating mechanism
180L/day 24L/day 36L/day 1.5L/day

15
Na balance Na+, K+-ATPase pump에 의해 Na+은 세포 밖으로 분비되어, 세포외액에 체내 85-90% Na+가 분포한다→ ECF volume=total body Na+ 반영. Na+ 농도(concentration)의 변화:수분 조절 이상 Na+ 함유량(content)의 변화: 체액량의 변화 Filtered Na+의 양: 180L/day x 140mmol = 25,200 mmol Na+ excretion; 100mmol/day
의 변화:수분 조절 이상. Na+ 함유량(content)의 변화: 체액량의 변화. Filtered Na+의 양: 180L/day x 140mmol = 25,200 mmol. Na+ excretion; 100mmol/day.")
17
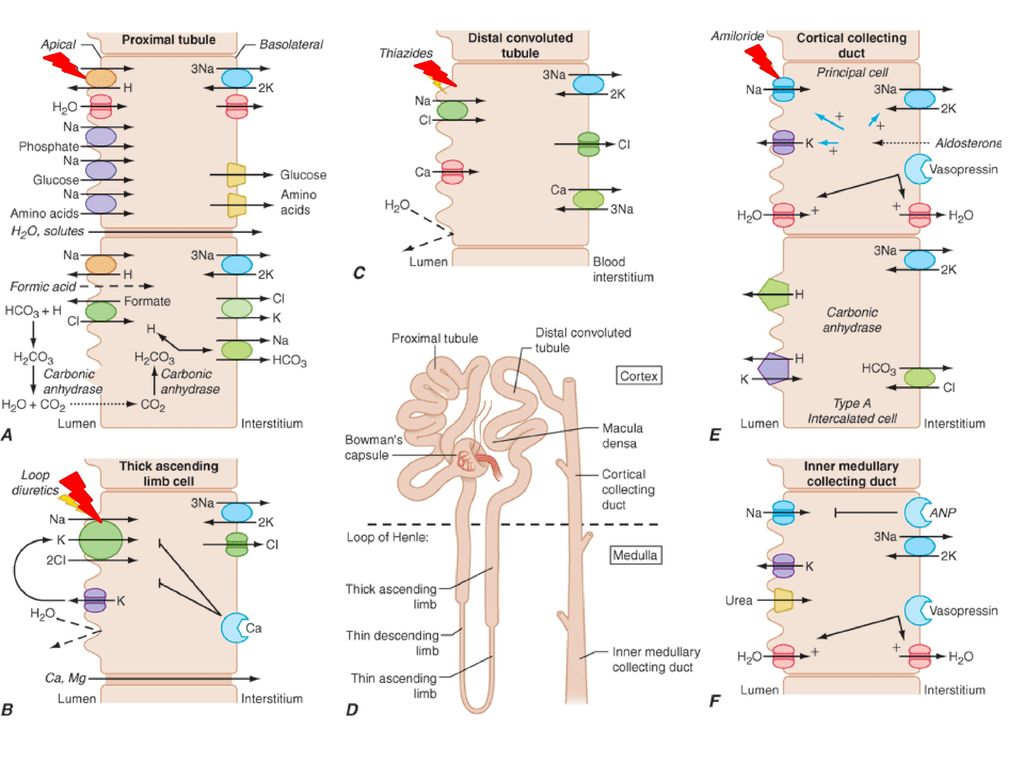
신장의 Na 재흡수 Angiotensin II Sympathetic tone↑ Dopamine

19
Circulatory integrity (순환량 보전)
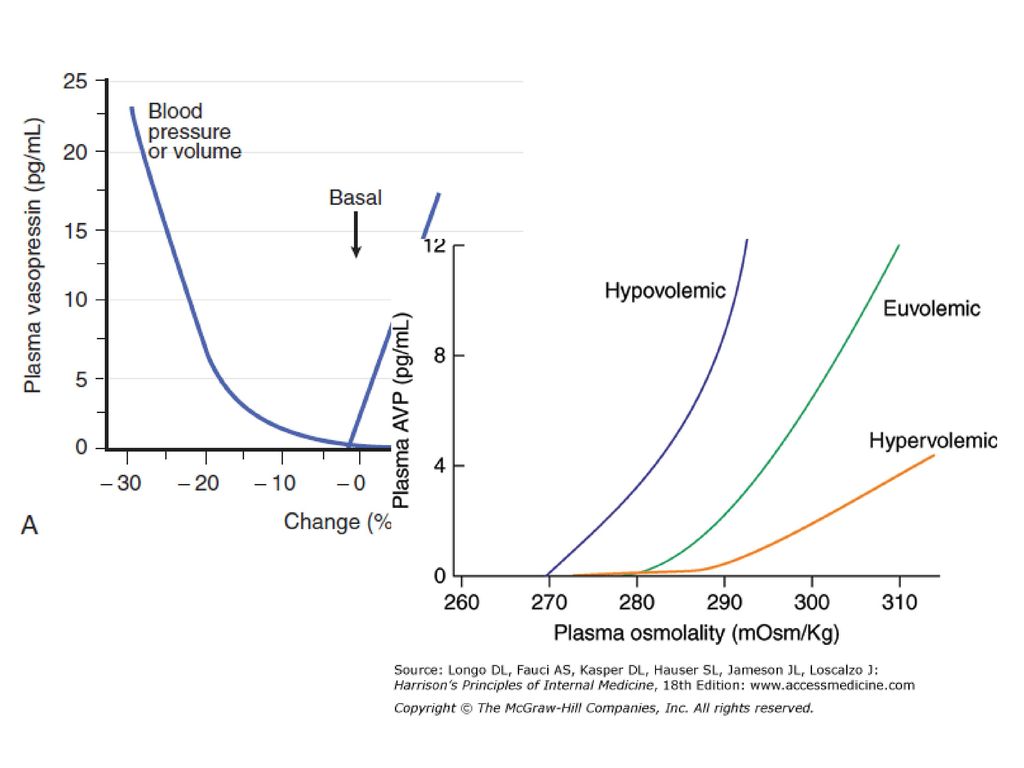
Vital organs에 prefusion & function을 위해 중요 Ventricular & vascular pressure receptor가 감지 Sympathetic tone↑,RAS activation, AVP↑

21
체액량 조절의 기전 AVP

22
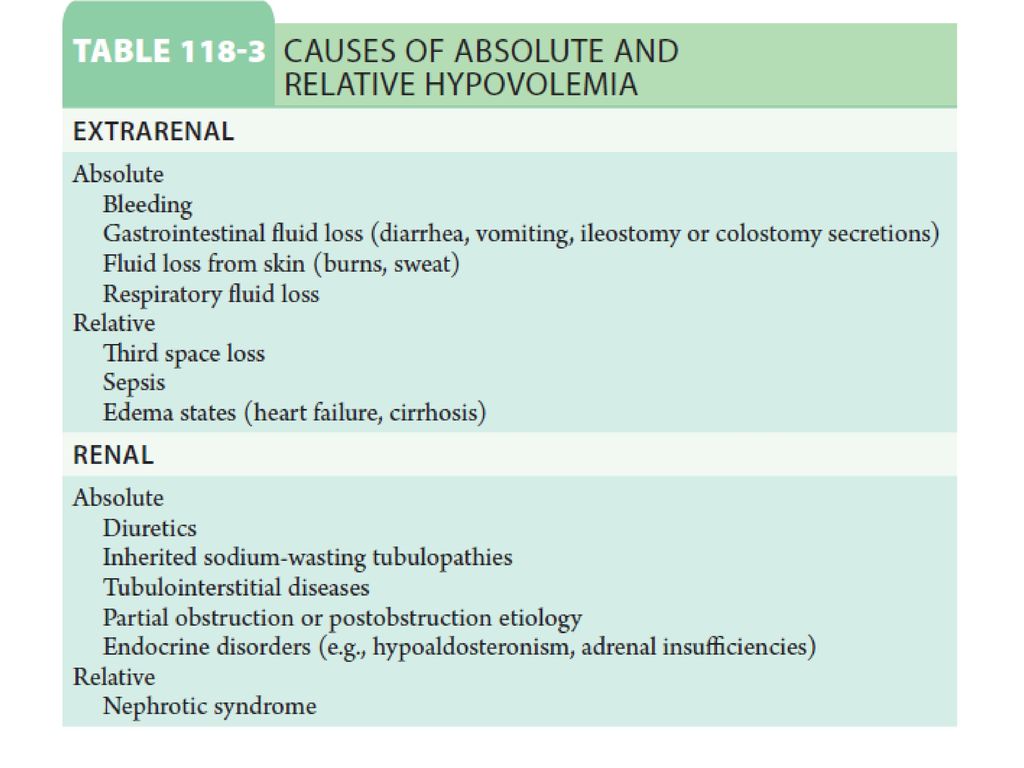
저체액상태 (Hypovolemia) (1) true hypovolemia:
총 체액량, 기능적 세포외 체액량 및 세포내 체액량이 모두 감소 수분과 소디움 (염분) 소실이 병합 (2) 순환장애에 의한 체액량의 이상 (circulatory compromised without external fluid loss)
 소실이 병합. (2) 순환장애에 의한 체액량의 이상 (circulatory compromised without external fluid loss)")
24
진단 Sx: non-specific → hypovolemic shock: hypotension, tachycardia, peripheral vasoconstriction, peripheral hypoperfusion Sign: JVP↓, orthostatic tachycardia & hypotension Hypovolemic shock-peripheral cyanosis, cold extrimites, oliguria, altered mentality

25
BUN과 Cr ↑, 사구체여과율↓. AVP↑, 콩팥의 소디움과 물의 재흡수 ↑, BUN/Cr 비: 10:1→ 20:1까지 상승 LFT, cardiac marker, blood gas 소변의 농축: Na+ < 20 mmol/L, osmolarity >450 mmol/Kg, specific gravity> 1.015 - Cl- <25mmol/L

26
치료 목표: 이미 손실된 체액에 맞게 양과 성분을 보충하고 지속되는 손실량만큼 보충해 체액의 상태를 정상화
(2) 체중: 체액 보충의 척도 (3) 수액 경도의 체액량 감소: 경구 투여, 저혈압/쇽 상태: 생리식염수 중증 저나트륨혈증: 고농도 생리식염수, 고나트륨혈증: half saline이나, dextrose M. acidosis: 5DW+150mEq Na-HCO3 심한 출혈이나 빈혈: 수혈, colloid solution (albumin,dextran)
 체중: 체액 보충의 척도. (3) 수액. 경도의 체액량 감소: 경구 투여, 저혈압/쇽 상태: 생리식염수. 중증 저나트륨혈증: 고농도 생리식염수, 고나트륨혈증: half saline이나, dextrose. M. acidosis: 5DW+150mEq Na-HCO3. 심한 출혈이나 빈혈: 수혈, colloid solution (albumin,dextran)")
27
Which fluid?

28
흔히 사용하는 수액제의 구성성분 Fluid Osmolarity (mosm/Kg) Glucose (mg/L)
Na+ (mEq/L) K+ (mEq/L) Cl- (mEq/L) 5% DW 252 50 10% DW 505 100 0.45% NaCl 154 77 0.9% NaCl 308 3% NaCl 1026 513 5% DS 560 Lactate Ringer’s 309 130 4 109
 K+ (mEq/L) Cl- (mEq/L) 5% DW % DW % NaCl % NaCl % NaCl % DS Lactate Ringer’s")
29
과체액상태 (Hypervolemia) Sodium retention
 Sodium retention")
30
진단 uNa ↓, FENA ↓ BNP↑ Sx: jugular venous distension, hypertension
periperal pitting edema (> 3L interstitial volume), ascites, pleural effusion uNa ↓, FENA ↓ BNP↑
, ascites, pleural effusion. uNa ↓, FENA ↓ BNP↑")
31
치료 Goal: ECF ↓, (-) Na balance Na restriction <20-40mmol/day
Diuretics-natriuretics nersiritide

32
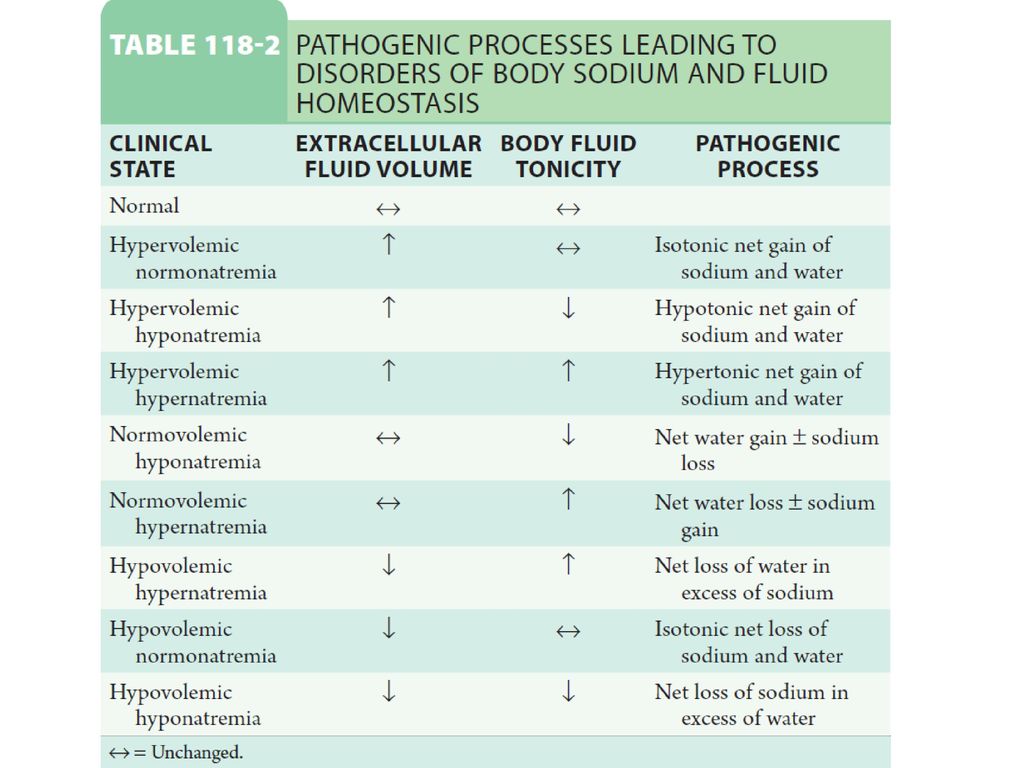
Na & water balance disorder
Water hemeostasis & total body Na+ Hyponatrema hypovolemia Hypernatremia hypervolemia Polyuria Serum osmolarity Water intake, circulating AVP

33
저나트륨혈증 (hyponatremia)
정의: 혈장 Na+ 농도 <135 mmol/L 입원환자의 22% Circulating AVP↑, AVP sensitivity↑

35
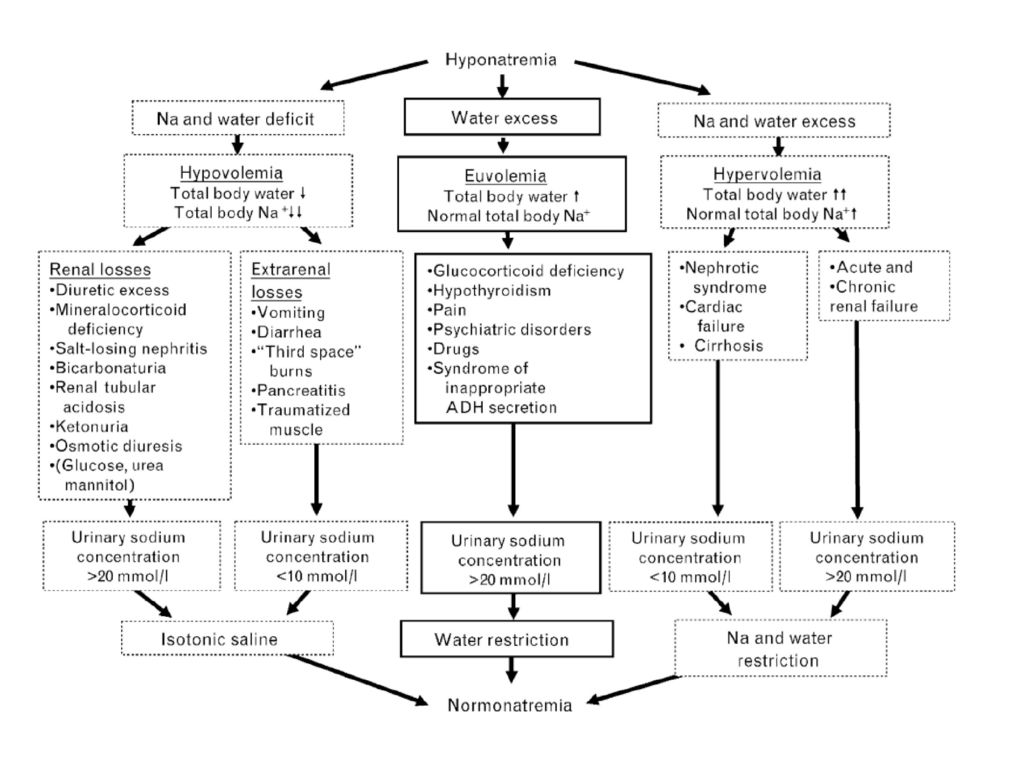
Hypovolemic hyponatremia
① Non-renal cause circulating AVP↑ →V1AR, V2R activation → urine Na+↓ <20mM ② Renal cause; urine Na+ >20mM thiazide계 이뇨제: Na+, K+의 결핍과 AVP↑의 물 저장효과 cf) loop계 이뇨제: 신수질 간질 부위의 삼투압을 감소시키고 요농축 기전을 억제하므로 AVP의 물 저장 효과를 억제 Cerebral salt wasting (renal salt wasting) urine Na+ >100mM Aggressive Na+-Cl- replacement
 loop계 이뇨제: 신수질 간질 부위의 삼투압을 감소시키고 요농축 기전을 억제하므로 AVP의 물 저장 효과를 억제. Cerebral salt wasting (renal salt wasting) urine Na+ >100mM. Aggressive Na+-Cl- replacement.")
36
Hypervolemic hyponatremia
Total body water↑↑> total body Na+-Cl- Acute or chronic renal failure : urine Na+ >20mM CHF, Cirrhosis, Nephrotic syndrome : urine Na+ < 10mM

37
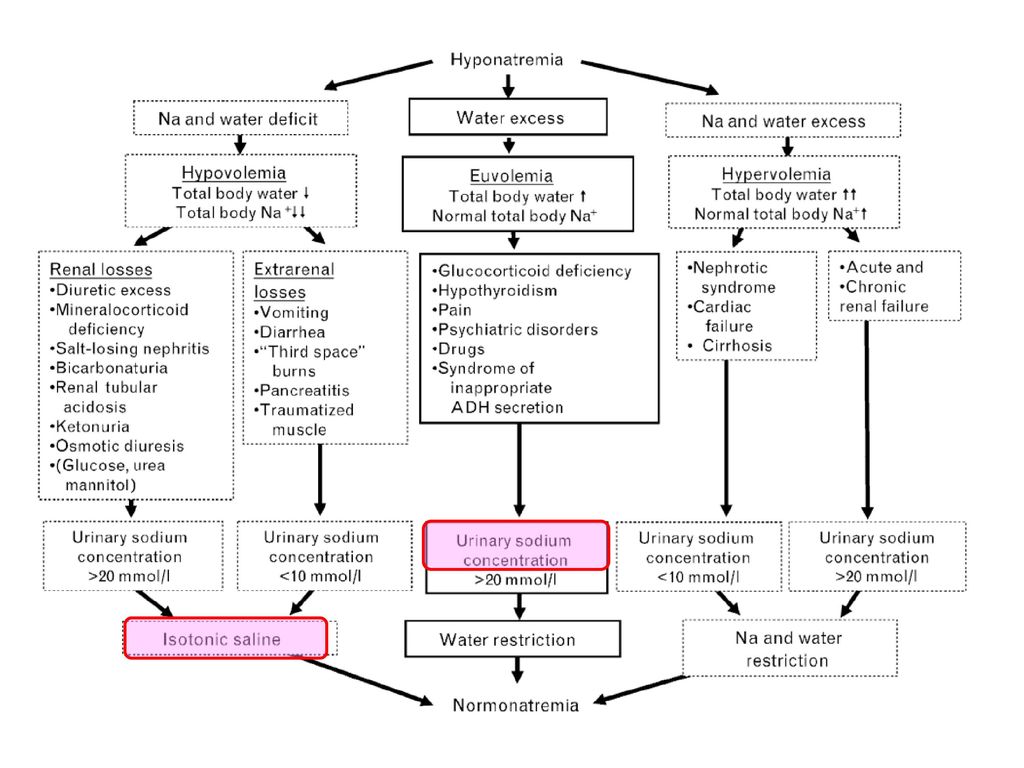
Euvolemic hyponatremia
부신 기능저하증 (glucocorticoid: AVP negative feedback) 갑상선 기능저하증 Stress Drug Syndrome of inappropriate antidiuretic hormone secretion
 갑상선 기능저하증. Stress. Drug. Syndrome of inappropriate antidiuretic hormone secretion.")
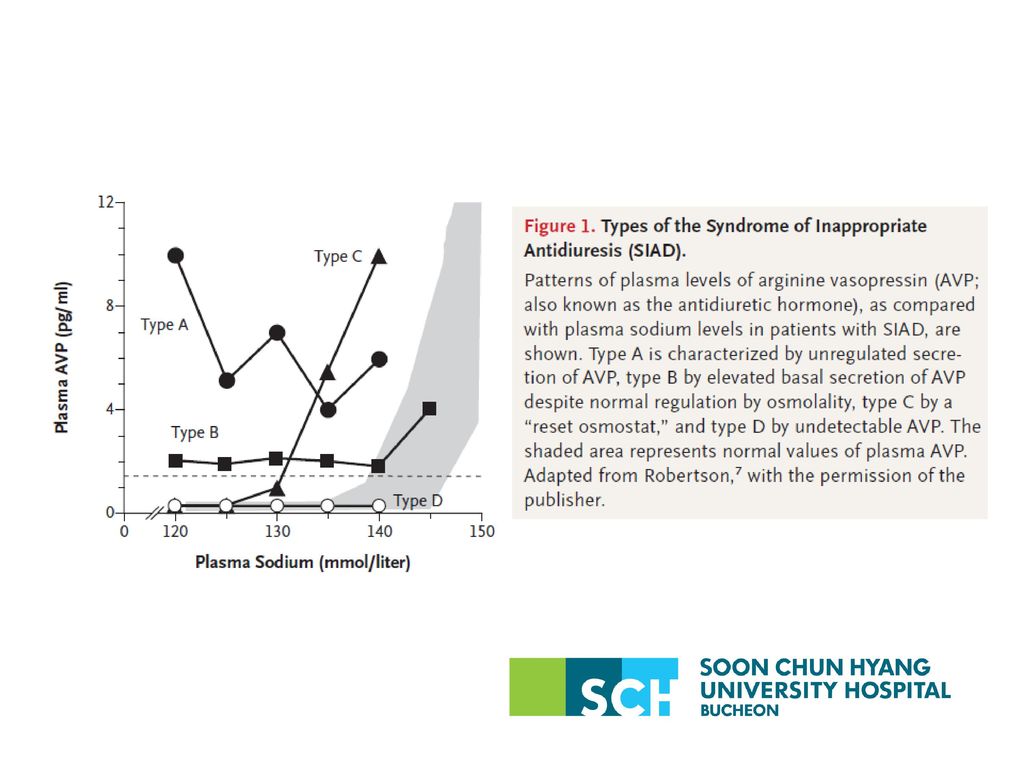
39
SIAD Distal tubular Na-Cl and water transport > proximal Na-Cl & urate transporter Uric acid <4mg/dL Pulmonary disease CNS disease Malignance (SCLC: 75%) SSRI
 SSRI.")
40
Case 2. 59세 남자(230552)로 1일 전부터 악화된 전신쇠약감과 발한으로 응급실 방문, 20년전 폐결핵 치료받았고, 10년 전부터 고혈압으로 복약중이며 하루 소중 2-3병의 음주하며 내원 1주전부터 소주만 마시다가 4일전부터 설사(3-4회/day)와 구토 있었음 BUN/Cr 10.7/1.0mg/dL Glucose 184mg/dL T.pro/alb 7.4/4.3g/dL Uric acid 8.9mg/dL GOT/GPT 140/73 IU/L Na/K/Cl/tCO2 119/2.6/71/31 mmol/L

41
1st admission urine Na/K 24/35.4 mmol/L Urine Osmolarity 407 mOsm/L
Serum osmolarity 243 mOsm/L

42
Second Adx Na/K/Cl/tCO2 115/3.8/77/26 mmol/L BUN/Cr 8.7/0.7 mg/dL
GOT/GPT 58/35 IU/L Uric acid 7.0 mg/dL urine Na 6 mmol/L Urine Osmolarity 43 mOsm/L Serum osmolarity 284 mOsm/L

43
Low solute intake and hyponatremia
V (Urine flow) = CH2O (free water clearance) +Cosm(solute clearance) (1) Cosm= Usom * V / Posm CH2O=V – Usom * V / Posm (2) V= solute excretion / Usom (3) (4) CH2O= Solute excretion (1- Uosm ) Posm Solute excretion (1- UNa+UK ) Uosm PNa
 = CH2O (free water clearance) +Cosm(solute clearance) (1) Cosm= Usom * V / Posm. CH2O=V – Usom * V / Posm (2) V= solute excretion / Usom. (3) (4) CH2O= Solute excretion. (1- Uosm. ) Posm. Solute excretion. (1- UNa+UK. ) Uosm. PNa.")
44
Low solute intake and hyponatremia
Solute excretion ∝ water clearance Urea balance-10g protein intake: 100mmol/d production: 50mmol/d excretion Beer potomania : low solute intake + high water intake If Usom 80moms, solute excretion 300mosm Water clearance= 300 * (1- 80 ) =2.7L
 =2.7L")
45
Berl. J Am Soc Nephrol 19: , 2008

46
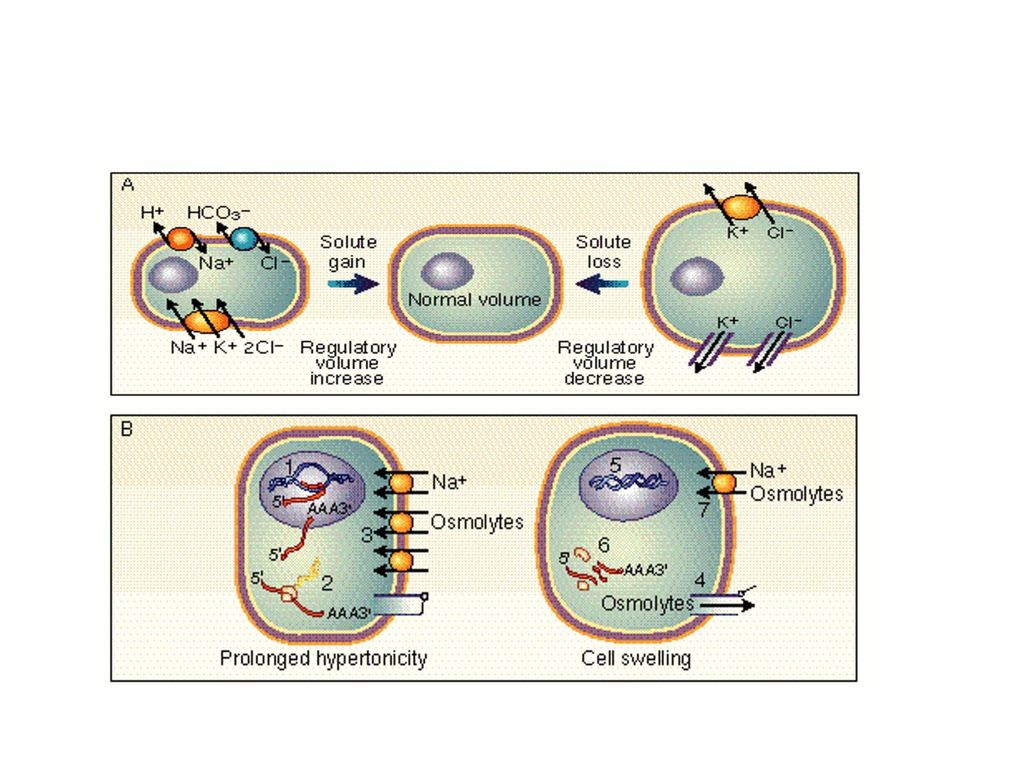
임상 증상 삼투압에 의해 세포내로 물이 유입되며, 특히 뇌세포에서는 뇌부종이 발생하여 신경학적 증상들이 나타나며,
Acute symptomatic Nausea, headache, vomiting Seizure, brain stem herniation, coma, death Normocarpnic respiratory failure Chronic Subtle gait, cognitive defect, bony Fx Reproductive women

47
<48hr efflux of creatine, betaine, glutamate, myo-inositol, taurine

48
진단 Chest PA Serum osmolarity, protein, lipid, glucose BUN/Cr, K
Uric acid LFT TFT Rapid ACTH stimulation test Urine Na, K, osmolarity Adrenal. Pituitary function

50
치료 (I) 1) 3 고려: Symptom, Speed, Monitor 2) Acute symptomatic
무증상: 치료 불필요 Risk of ODS: >8-10mM first 24hr,>18mM first 48hr frequent monitoring 2) Acute symptomatic 1-2mM/h to 4-6mM, 3% NS 부족한 Na+량=(140-혈청 Na+) * 전신 총 수분량 2-4hr monitoring IV lasix; pulmonary edema
 Acute symptomatic. 1-2mM/h to 4-6mM, 3% NS. 부족한 Na+량=(140-혈청 Na+) * 전신 총 수분량. 2-4hr monitoring. IV lasix; pulmonary edema.")
51
치료 (II) 3) Chronic <8-10mM first 24hr,<18mM first 48hr
Underlying cause ① 세포외액 감소 시: Na+ 투여 (생리식염수) -혈장 Na+ 미치는 효과는 적으나, AVP의 분비↓, free water의 배설 ↑ ② 세포외액 증가한 부종 시: -수분 (total body water) > 염분 (total body Na+), 염분과 수분 섭취을 제한하고 (소변량보다 적게), 저칼륨혈증을 교정하고, 염분보다 수분을 더 많이 배설 (loop계 이뇨제) ③ Vaptan
 -혈장 Na+ 미치는 효과는 적으나, AVP의 분비↓, free water의 배설 ↑ ② 세포외액 증가한 부종 시: -수분 (total body water) > 염분 (total body Na+), 염분과 수분 섭취을 제한하고 (소변량보다 적게), 저칼륨혈증을 교정하고, 염분보다 수분을 더 많이 배설 (loop계 이뇨제) ③ Vaptan.")
52
치료 (III) Vasopressin antagonist
10%; overcorrect, if non-liberal water intake Demopressin+ free water

53
Case 3. 54세 남자로 수일 전부터 사지의 화끈거리는 느낌으로 응급실 방문, 특별한 과거력 없음
BUN/Cr 14.1/1.0mg/dL Glucose 115 mg/dL T.pro/alb 7.4/4.8g/dL Uric acid 3.3 mg/dL GOT/GPT 43/20 IU/L CK 1149 IU/L, myoglobin 269 ng/dL Na/K/Cl/tCO2 120/4.0/88/22 mmol/L

54
Urine Osmolarity 634 mOsm/L Serum osmolarity 255 mOsm/L
urine Na 115 mmol/L Urine Osmolarity 634 mOsm/L Serum osmolarity 255 mOsm/L HAD 1 2 3 4 5 6 7 sNa 120 116 123 126 128 129 uNa 115 147 187 241 278 328 sOsm 255 uOsm 634 474 538 622 589 670 694 Urine Output(mL) 2270 1760 850 1120 1750 3780 3230
")
56
NEJM 356: , 2007

57
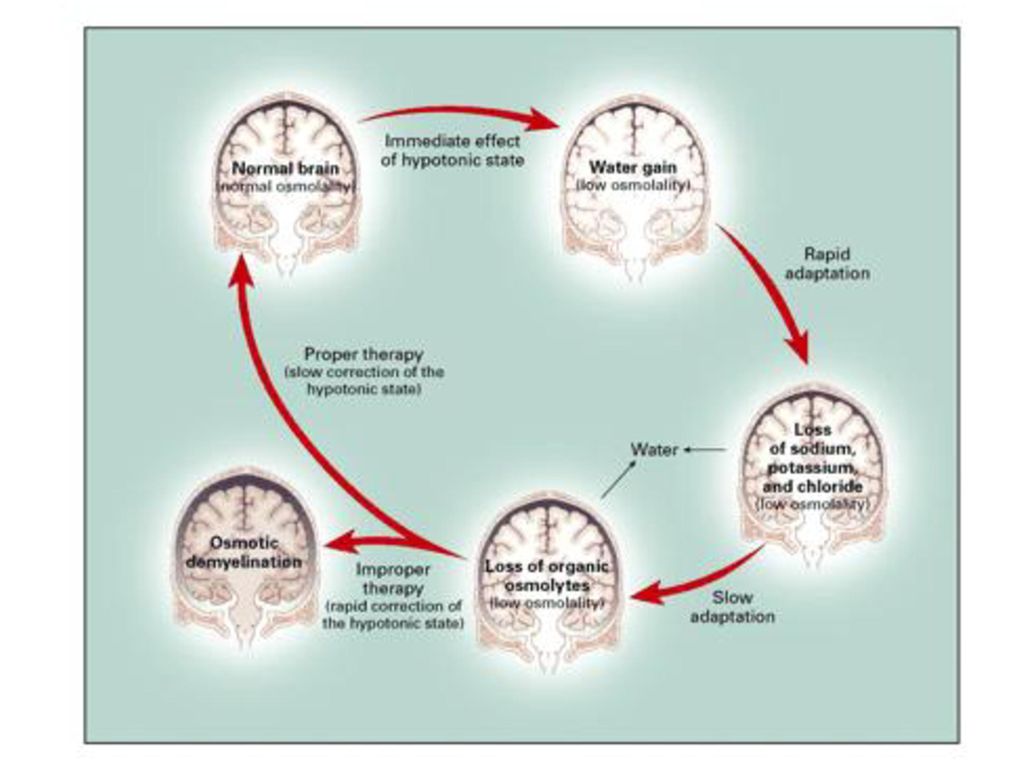
삼투성 탈수초 증후군 (osmotic demyelination syndrome)
너무 빠른 교정 시: Para- or quardraparesis, 구음장애, diplopia, locked-in syndrome, 의식소실 Ataxia, mutism, parkinsonism, dystonia, catatonia Pons > cerebellum, thalamus, putamen, cortex 임상적으로 진단, MRI 등으로 확진. high risk: 저칼륨혈증, 영양실조, 알코올리즘 Liver transplantation

59
Case 4. 55세 남자로 내원 당일 발생한 의식저하로 응급실 방문, 특별한 과거력 없음
BUN/Cr 16.4/1.1 mg/dL Glucose 174 mg/dL T.pro/alb 7.3/4.4g/dL Uric acid 6.0 mg/dL GOT/GPT 33/31 IU/L Na/K/Cl/tCO2 139/3.3/101/14 mmol/L

60
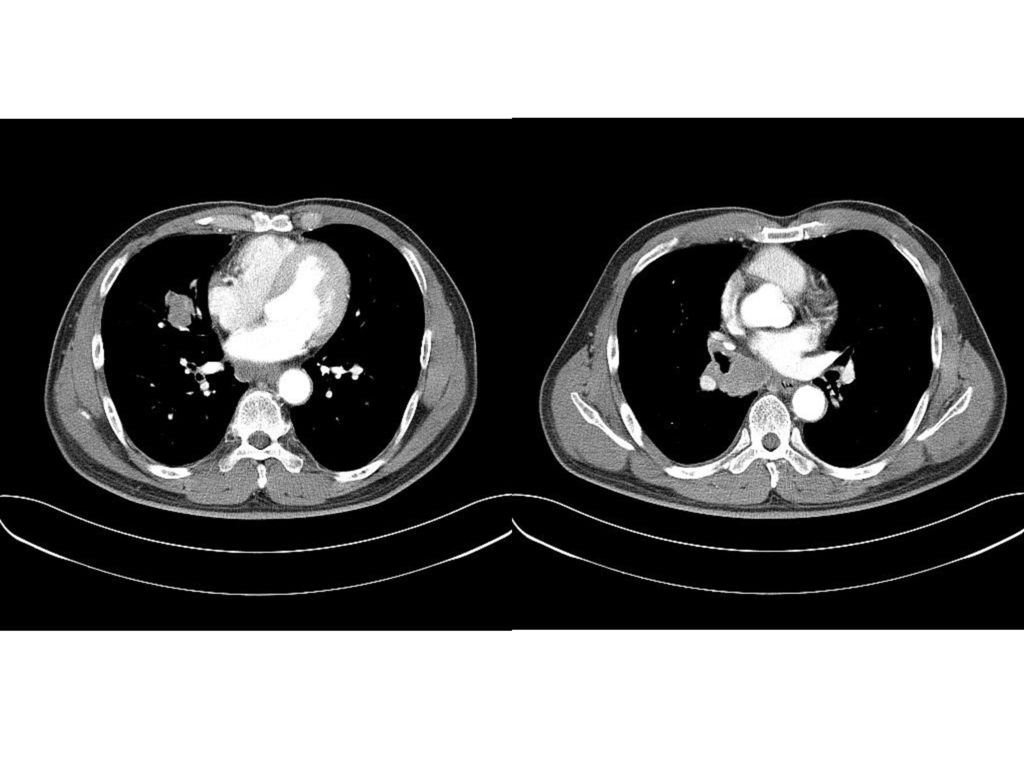
Thalamus

61
HAD 1 2 3 4 5 6 9 BUN 16.4 24.3 32.7 41 46.5 47 48 Cr 1.1 1.7 1.8 1.6 1.5 1.4 1.3 sNa 139 142 145 148 151 156 162 uNa 8 18 97 sOsm 308 314 325 335 341 344 uOsm 355 474 488 535 452 466 464 Urine Output(mL) 1540 2835 3515 3910 3750 2810 2915
")
62
고나트륨혈증 (hypernatremia)
정의: 혈장 Na+ 농도 >145 mmol/L Less common than Hyponatremia 40-60% mortality

63
원인 I. Impaired thirst Coma , Essential hypernatremia
II. Solute diuresis; osmotic diuresis Diabetic ketoacidosis, non-ketotic hyperosmolar coma, mannitol administration excess urea, postobstructive diuresis, III. Excessive water loss Renal: Central (pituitary) DI Nephrogenic DI: hypercalcemia, hypokalemia, lithium, ifosfamide Insensible loss; fever, exercise, heat exposure, burn, ventilator Diarrhea
 DI. Nephrogenic DI: hypercalcemia, hypokalemia, lithium, ifosfamide. Insensible loss; fever, exercise, heat exposure, burn, ventilator. Diarrhea.")
64
임상양상 감소한 뇌세포 용적은 뇌실질 출혈, SAH의 위험도를 높인다. Hypernatremic rhabdomyosis
의식의 저하, 쇠약감,→ deep coma 만성 고나트륨혈증에서는 삼투적응에 의해 대부분 증상이 없다.

65
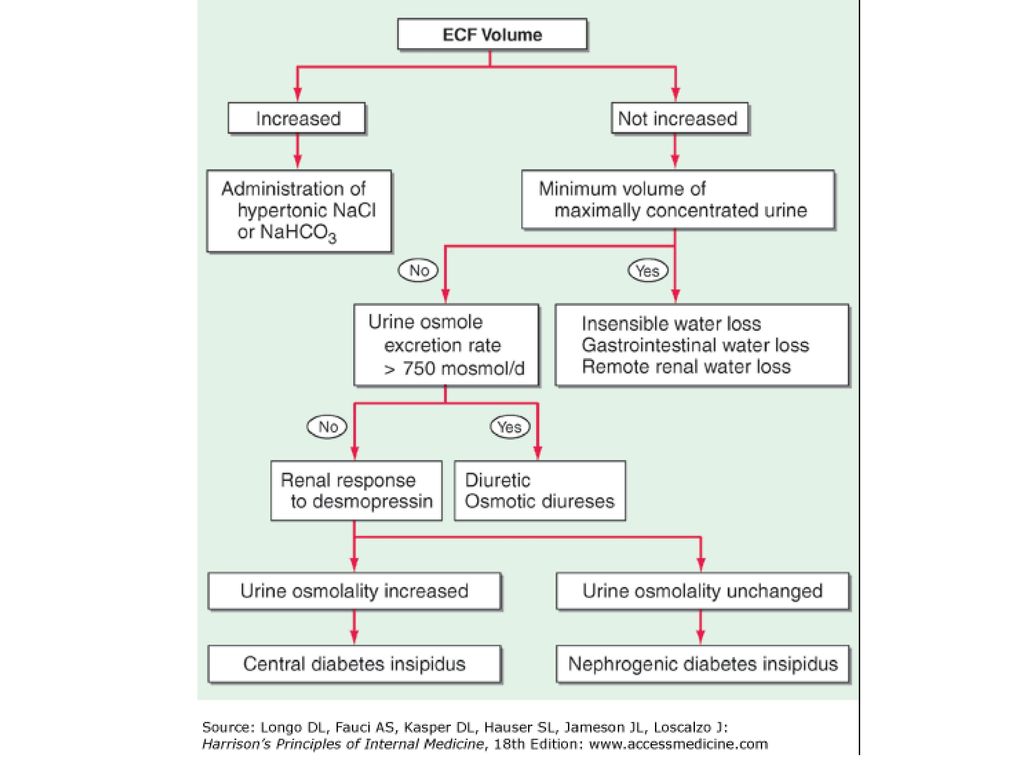
진단 (I) (1) 신장 정상: 최대한 농축 소변을 배설 소변 삼투질 농도 >800 mosmol/kg
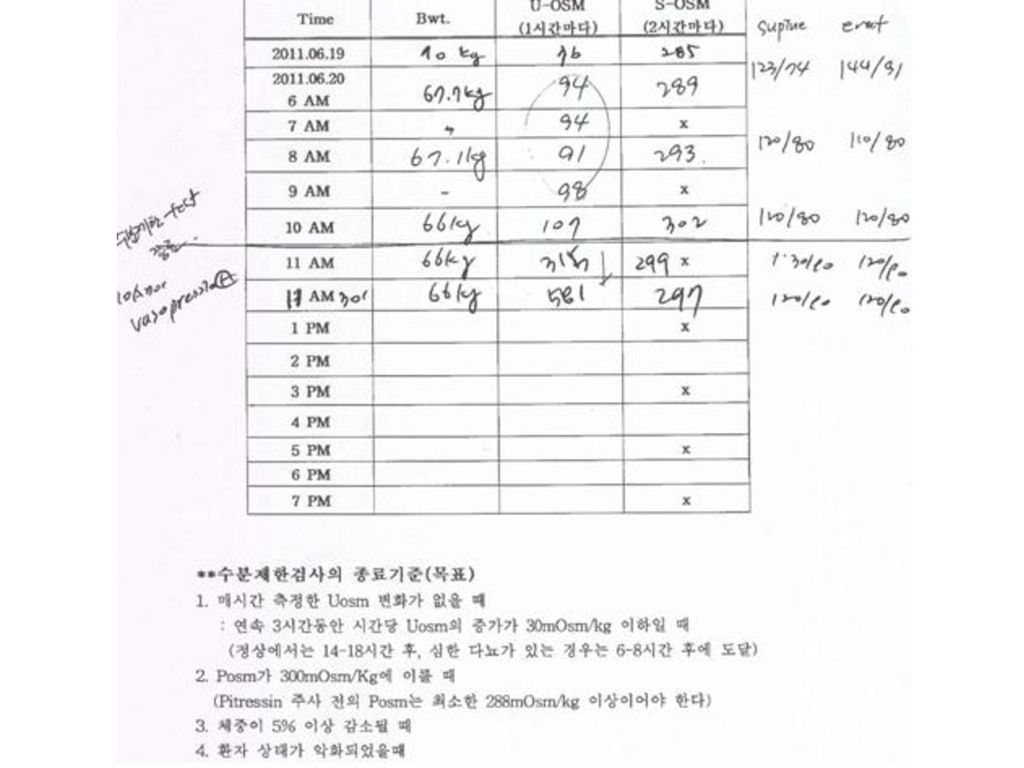
최소 소변양 (500 ml/day) 콩팥 이외, 고장성 Na+투여가 원인. (2) 일차적 Na+ 과다: 세포외액의 팽창과 natriruesis (소변 Na+ >100 mmol/L) (3) 삼투성 이뇨: 소변의 삼투질농도 > 750 mosmol/L 소변의 당과 요소 (urea)를 측정 (4) 요붕증: 다뇨와 저장성 소변(urine osmolarity < 250 mosmol/L) Water deprivation test 후에 AVP analogue desmopressin을 10 g을 비강내 투여하여 소변의 삼투질 농도가 50%이상 상승하면 중추성으로 그렇지 않으면 신성 요붕증으로 감별 진단.
 콩팥 이외, 고장성 Na+투여가 원인. (2) 일차적 Na+ 과다: 세포외액의 팽창과 natriruesis (소변 Na+ >100 mmol/L) (3) 삼투성 이뇨: 소변의 삼투질농도 > 750 mosmol/L. 소변의 당과 요소 (urea)를 측정. (4) 요붕증: 다뇨와 저장성 소변(urine osmolarity < 250 mosmol/L) Water deprivation test 후에 AVP analogue desmopressin을 10 g을 비강내 투여하여 소변의 삼투질 농도가 50%이상 상승하면 중추성으로 그렇지 않으면 신성 요붕증으로 감별 진단.")
67
치료 목표: (2) 수분 부족량 = (혈장 Na+ 농도-140)/140 * 전신 총 수분량
원인질환을 찾아 수분 손실을 막고, 부족한 수분양을 보충. water deficit+ ongoing water loss+ insensible loss (2) 수분 부족량 = (혈장 Na+ 농도-140)/140 * 전신 총 수분량 (3) 48-72시간 동안 천천히 교정. 교정 속도는 0.5 mmol/L/hr, 첫 24시간 내에 10 mmol이하로 교정. 물의 보충은 먹거나 비위관 투여가 가장 안전. 차선책으로 5% 포도당 용액, half-saline IV.
 수분 부족량. = (혈장 Na+ 농도-140)/140 * 전신 총 수분량. (3) 48-72시간 동안 천천히 교정. 교정 속도는 0.5 mmol/L/hr, 첫 24시간 내에 10 mmol이하로 교정. 물의 보충은 먹거나 비위관 투여가 가장 안전. 차선책으로 5% 포도당 용액, half-saline IV.")
70
Potassium Balance Major Intracellular cation: 150 mmol/L
Normal plasma K+ :3.5~5.0 mmol/L K+ in ECF: mmol/L Total body K+: mmol/L Principle results of the resting potential membrane (Na+-K+-ATPase in a 3:2) Crucial for neuromuscular function.
 Crucial for neuromuscular function.")
71
Stay hungry! Stay foolish!
70Kg 남자 ECF의 K양?

72
체내 K+ 분포 Internal balance External balance

73
Normal K balance Internal balance B2-adrenergic Thyroid H insulin
External balance

74
Case 5. 36세 여자로 3일전부터 발생한 구토와 전신 쇠약감으로 응급실 방문, BP 120/70mmHg, 10년 전 갑상선 저하증으로 2년간 복약함
BUN/Cr 13/0.9 mg/dL Glucose 155mg/dL T.pro/alb 8.2/4.4g/dL Uric acid 3.0 mg/dL GOT/GPT 35/63 IU/L Na/K/Cl/tCO2 134/1.8/109/14 mmol/L Mg 2.3mg/dL CK 245 IU/L, myoglobin 397 ng/dL

75
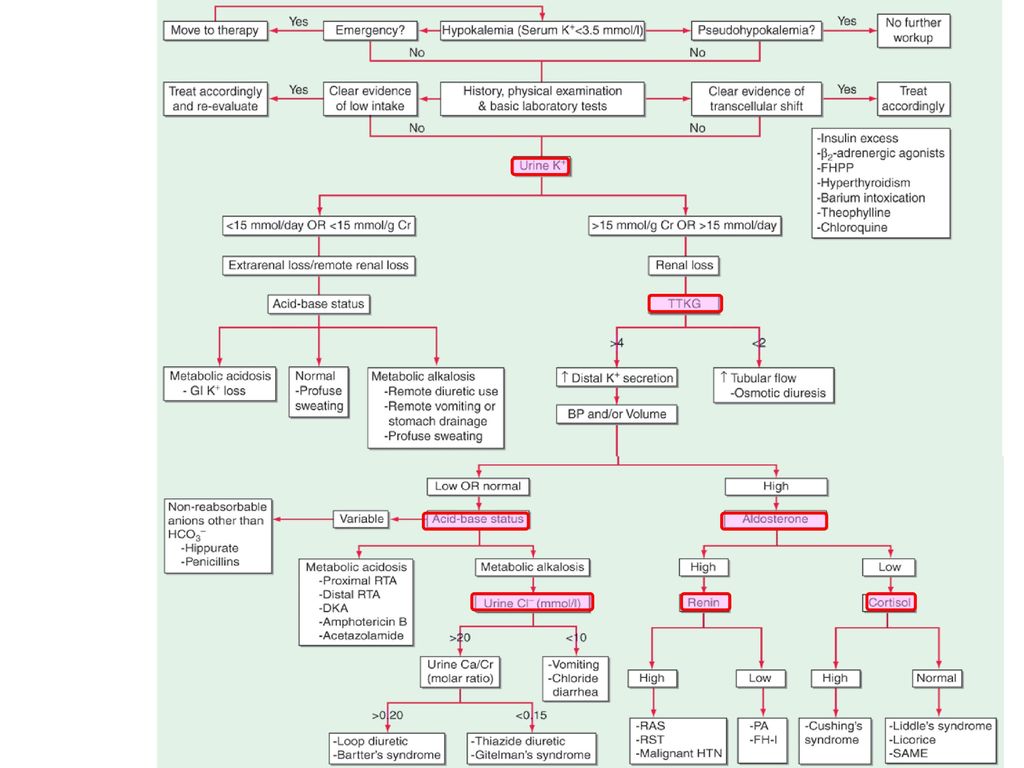
정의: 혈장 K+ 농도 <3.6 mmol/L 20% In hospitalized pt Mortality 10↑
저칼륨혈증 (hypokalemia) 정의: 혈장 K+ 농도 <3.6 mmol/L 20% In hospitalized pt Mortality 10↑
 정의: 혈장 K+ 농도 <3.6 mmol/L. 20% In hospitalized pt. Mortality 10↑")
76
원인

77
The renal concentrating mechanism
180L/day 24L/day 36L/day 1.5L/day

79
mmol/L mmol/L mmol/L

80
임상증상 (I) Cardiac, skeletal, intestinal effect
No symptoms if plasma K+< 2.7 mmol/L Fatigue, myalgia, muscular weakness of the lower extremities Rhabdomyolysis, paralytic ileus are common complaints and are due to a lower (more negative) resting membrane potential. (due to respiratory muscle involvement), Impaired muscle metabolism and the blunted hyperemic response to exercise associated with profound K+ depletion increase the risk of Smooth-muscle function may also be affected and manifest as
 resting membrane potential. (due to respiratory muscle involvement), Impaired muscle metabolism and the blunted hyperemic response to exercise associated with profound K+ depletion increase the risk of. Smooth-muscle function may also be affected and manifest as.")
81
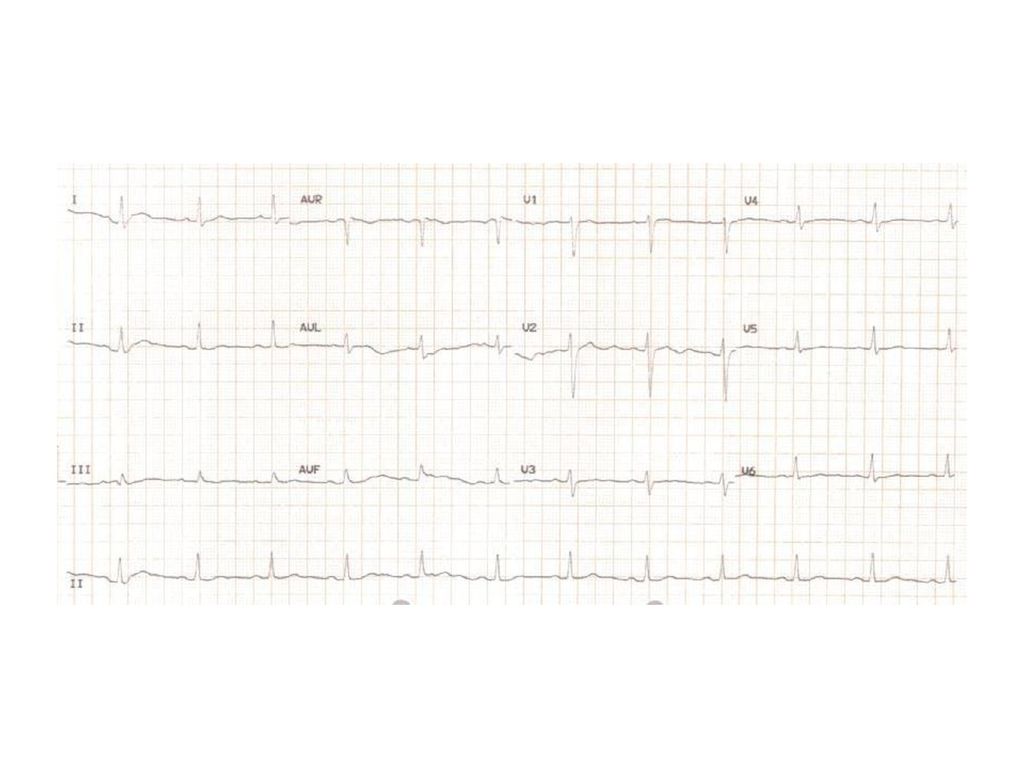
임상증상 (II) Early change Severe K depletion
Flattening or inversion of T wave ST segment depression Prolonged QT interval Severe K depletion Prolonged PR interval voltage↓ widening of QRS Ventricular arrhythmia

82
진단 Medication, BP, heart rate, ECF volume Muscle strength & reflex
Na, Cl, HCO3, BUN/Cr, aBGA, Creatine kinase, Mg EKG

84
Urine K 5.8 mmol/L Urine Osmolarity 182 mOsm/L Serum osmolarity 296 mOsm/L aBGA: % Urine pH 7.5, RBC<1, WBC<1, alb(-) FreeT ng/dL TSH uIU/mL
 FreeT ng/dL. TSH uIU/mL.")
86
치료 (I) Goal: oral route 가 안전, plasma K+ 자주 check!
prevent life-threatening ± chronic consequence Replace K deficit Correct underlying causes± mitigate future loss oral route 가 안전, plasma K+ 자주 check! 0.27mM↓ for every 100mM 1 mmol/L in the plasma K+ (from 4.0 to 3.0 mmol/L) = total body K+ deficit of 200–400mmol due to insulin-mediated movement of K+ into cells.
 = total body K+ deficit of 200–400mmol. due to insulin-mediated movement of K+ into cells.")
87
치료 (II) NS > DW mix KCl
The maximum concentration of administered K+ 40 mmol/L via a peripheral vein →phlebitis, irritation, sclerosis ② 60 mmol/L via a central vein. Speed :20 mmol/h 초과하지 않기!

88
Case 6. 61세 여자로 1일전부터 발생한 호흡곤란과 흉통으로 응급실 방문, BP 120/70mmHg, 심박수 48회, 25년 전 당뇨, 고혈압과 심부전으로 복약 중
BUN/Cr 41/1.6 mg/dL Glucose 131mg/dL T.pro/alb 8.0/4.7g/dL Uric acid 8.1 mg/dL GOT/GPT 22/25 IU/L Na/K/Cl/tCO2 135/8.0/103/23 mmol/L CK-MB 2.5 IU/L, myoglobin 56.8 ng/dL, troponinT<0.01

89
정의: 혈장 K+ 농도 >5.5 mmol/L 10% of hospitalized pts
고칼륨혈증 (hyperkalemia) 정의: 혈장 K+ 농도 >5.5 mmol/L 10% of hospitalized pts
 정의: 혈장 K+ 농도 >5.5 mmol/L. 10% of hospitalized pts.")
90
원인

91
임상증상 Heart: Neuromuscular Sx
Sinus bradycardia, ventricular fibrillation, asystole Neuromuscular Sx Weakness: flaccid paralysis, hypoventilation Paresthesia Dizziness Muscle cramps Renal Amoniagenesis inhibition Metabolic acidosis K의 신장에서의 조절은 cells of the cortical collecting duct에서 조절된다 amiloride-sensitive epithelial sodium channel (ENaC)을 통하여 Na이 분비되고 그에따라 lumen 내에 negative potential 이 발생하여 K이 K+ channel ROMK 을 통하여 lumen 내로 분비되게 된다. Flow-dependent K+ secretion is thought to be mediated by an apical, voltage-gated, calcium-sensitive maxi-K channel. 91
을 통하여 Na이 분비되고 그에따라 lumen 내에 negative potential 이 발생하여 K이 K+ channel ROMK 을 통하여 lumen 내로 분비되게 된다. Flow-dependent K+ secretion is thought to be mediated by an apical, voltage-gated, calcium-sensitive maxi-K channel. 91.")
92
EKG 변화 K concentration EKG change 4 Normal 5.5-6.5 Tall peaked T wave
Loss of P waves 7-8 Widened QRS >8 Sine wave

93
Urine K 31.1 mmol/L Urine Osmolarity 337 mOsm/L Serum osmolarity 296 mOsm/L aBGA: % Urine pH 7.0, RBC<1, WBC<1, alb(-) FreeT ng/dL TSH uIU/mL
 FreeT ng/dL. TSH uIU/mL.")
94
진단

95
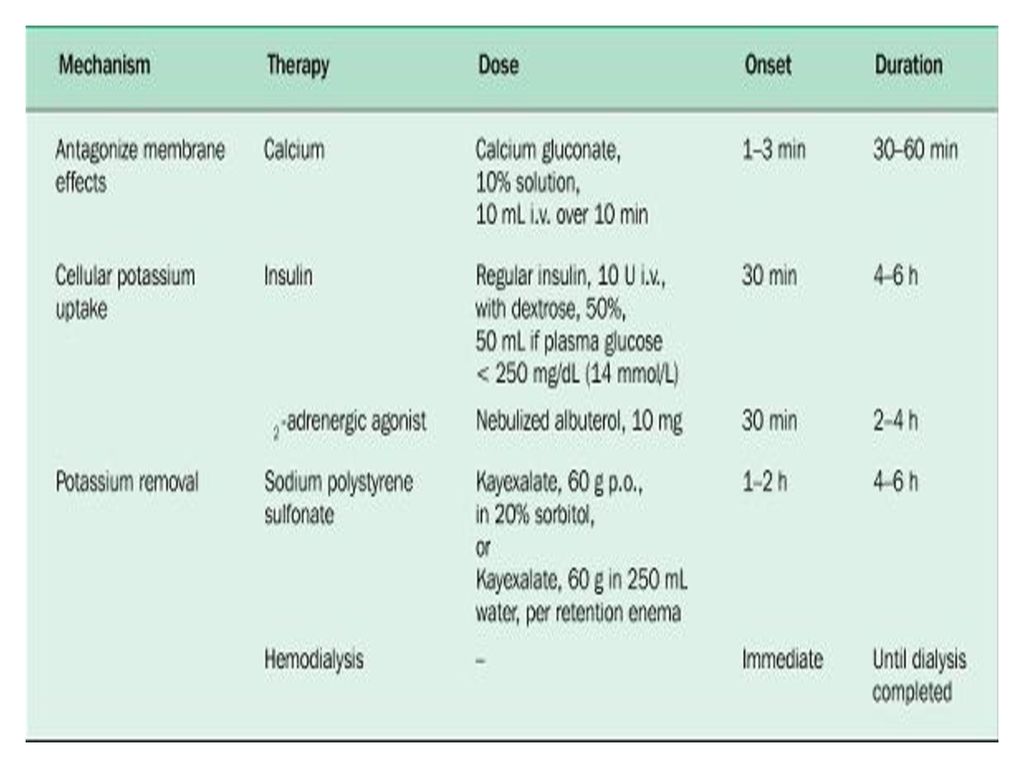
치료 minimizing membrane depolarization
10% calcium gluconate 10mL IV over 2-3 min Digoxin 사용 시 hypercalcemia risk↑로 5DW 100cc에 mix해서 30분 이상 infusion Shifting K+ into cells 50% DW 50cc + RI 10u If hypoglycemia→ 10DW 50-75ml/min If glucose > mg/dL→ insulin β2-adrenergic agonist 흡입 Inhaled ambuterol 10-20mg+NS 4cc

96
치료 II NaHCO3: M. acidosis Direct K + removal from body
Sodium polystyrene sulfonate(SPS) enema 15-30g +33% sorbitol-> lactulose, polyethylen glycol 3350 intestitinal necrosis ② Loop and thiazide diuretics ③ Dialysis
 enema g +33% sorbitol-> lactulose, polyethylen glycol intestitinal necrosis. ② Loop and thiazide diuretics. ③ Dialysis.")
98
Thank you!

Similar presentations



 란 ? 1) 넓은 의미 order 문서보고 2) 좁은 의미 ; 1 시간 검사실 검체 접수 문서보고.>")
 3 days ago CC: Feveronset) 3 days ago PI : F/29, 5 년전 첫아기 임신 8 개월째에.>")














