Download presentation
Presentation is loading. Please wait.

1
Biologic therapy in the rheumatic disease 경희의료원 류마티스내과 이연아

2
Contents Definition, Nomenclature of biologic agents Blocking cytokine activity TNF-α : infliximab, adalimumab, etanercept, golimumab, certolizumab Indication, Switching latent Tbc screening IL-1: anakinra, rilonacept IL-6: tocilizumab Co-stimulation blockade CTLA-4 : abatacept B-cell depletion CD 20 : rituximab

3
Paradigm Shift : treatement of rheumatic diseases EmpiricalEvidence -basedMechanism-based 1940-50s Aspirin Gold Steroids 1970-90s NSAIDs MTX Cytotoxic agents 1998-Current Cox-2 inhibitors Biologic (ex: mAb)
")
4
Definition of Biologic agent A substance that is made from a living organism or its products and is used in the prevention, diagnosis, or treatment of cancer and other diseases. Biologics 의 특징 Protein-based, made by biological technology Specific effects: neutralise or block the target molecules (cell surface marker, proinflammatory cytokine) High efficacy include antibodies, interleukins, and vaccines.
 High efficacy include antibodies, interleukins, and vaccines..")
5
생물학적제제 특성

6
Strategies of cytokine inhibition 1. Monoclonal Ab- Infliximab, Adalimumab 2. Soluble receptor- Etanercept 3. Receptor antagonist- Anakinra 4. Receptor mAb- Tocilizumab NEJM, Vol. 344, 2001 1. 2. 3. 4.

7
Nomenclature of monoclonal Ab Source substems: mouse (top left), chimeric (top right) : constant region 이 human form humanized (bottom left) : complementarity determining region(CDR) 을 제외한 variable regions 이 human form 으로 되어 있는 것 chimeric/humanized (bottom middle) human monoclonal Ab (bottom right) human parts: red, non-human parts: blue
, chimeric (top right) : constant region 이 human form humanized (bottom left) : complementarity determining region(CDR) 을 제외한 variable regions 이 human form 으로 되어 있는 것 chimeric/humanized (bottom middle) human monoclonal Ab (bottom right) human parts: red, non-human parts: blue")
8
Adalimumab :ada- lim -u -mab Infliximab : Inf- li -xi -mab Prefix+target substem+source substem+suffix

9
Expert Opin. Pharmacother. 2007; 8(14):2371-79 Inflammatory cells and cytokines
: Inflammatory cells and cytokines")
10
TNF-alpha blocking agents

11
Cytokines balance Pro-inflammatory Anti-inflammatory TNF IL-1 sTNFR IL-4,10 TGF-β IL-1Ra 종양괴사 인자 (TNF-α) - 류마티스 관절염에서 가장 중요한 염증 매개 물질 - 관절 부종과 통증같은 염증반응과 연골 및 골파괴 일으킴
 - 류마티스 관절염에서 가장 중요한 염증 매개 물질 - 관절 부종과 통증같은 염증반응과 연골 및 골파괴 일으킴")
12
종양괴사인자 (TNF - ) 종양괴사인자 (TNF - ) 류마티스 질환에서 중요한 병인 대식세포 내피세포 간세포 활막세포 염증성 사이토카인 케모카인 부착인자 급성기 단백 Metalloproteinase 합성 VEGF 관절연골 손상 CRP 증가 혈관 신생 염증세포 침윤 염증 증가 전구 파골세포 RANKL 발현 골미란 종양괴사인자
 종양괴사인자 (TNF - ) 류마티스 질환에서 중요한 병인 대식세포 내피세포 간세포 활막세포 염증성 사이토카인 케모카인 부착인자 급성기 단백 Metalloproteinase 합성 VEGF 관절연골 손상 CRP 증가 혈관 신생 염증세포 침윤 염증 증가 전구 파골세포 RANKL 발현 골미란 종양괴사인자")
13
TNF-alpha 차단제 종류 - 염증 반응의 중추적 물질인 종양괴사인자 중화 -RA 치료에서 MTX 와 병합 사용하면 강력한 효과 infliximab (remicade ® ) etanercept (enbrel ® ) adalimumab (humira ® ) 키메라 단클론 TNF- - 항체 p75- 인간 TNF 수용체 -IgG1-Fc- 융합단백 인간 단클론 TNF- - 항체 인간 IgG1-Fc- 부분 특이적 결합 부위
 etanercept (enbrel ® ) adalimumab (humira ® ) 키메라 단클론 TNF- - 항체 p75- 인간 TNF 수용체 -IgG1-Fc- 융합단백 인간 단클론 TNF- - 항체 인간 IgG1-Fc- 부분 특이적 결합 부위")
14
50-100mg s.c monthly TNF-alpha 차단제 종류

15
Etanercept : Mode of Action sTNFR:Fc sTNFR:Fc ( 엔브렐 )
")
16
Infliximab / Adalimumab : Mode of Action Activated M M Target Cell Signal TNF TNFR

17
Pharmacokinetics of TNF inhibitors EtanerceptInfliximabAdalimumab Half-life (days) 59±116±2 Bind lymphotoxin o XX Bolus effectX o X Fix complementX oo Lyse cellsX oo Reversible binding o XX
 59±116±2 Bind lymphotoxin o XX Bolus effectX o X Fix complementX oo Lyse cellsX oo Reversible binding o XX")
18
in RA MTX, SSZ, leflunomide 등과 병용가능 MTX naïve 환자에서 first DMARD 로도 가능 Etanercept, Adalimumab : monoTx 로 가능하나 Infliximab 은 반드시 MTX 와 병용 (inhibiting Ag, HACA 생성을 억제함 ) MTX 와 combination 할 때 각각 사용하는 것보다 월등한 효과 골파괴 진행 억제 Onset time of action : within 12-24 주 in PsA Etanercept, Adalimumab, Infliximab, Golimumab monoTx or MTX combination Consensus statement on TNF blocking agent
 MTX 와 combination 할 때 각각 사용하는 것보다 월등한 효과 골파괴 진행 억제 Onset time of action : within 주 in PsA Etanercept, Adalimumab, Infliximab, Golimumab monoTx or MTX combination Consensus statement on TNF blocking agent")
19
류마티스 관절염 치료 전략의 변화 질병 활성도 (%) 증상 발현후 기간 ( 개월 ) 과거 증상 발현후 기간 ( 개월 ) 질병 활성도 (%) 최근 관절 손상 “ 조기에 적극적 치료 !” 조기에 항류마티스 약물 사용 단독보다 병합요법 단계적 약물 추가
 증상 발현후 기간 ( 개월 ) 과거 증상 발현후 기간 ( 개월 ) 질병 활성도 (%) 최근 관절 손상 조기에 적극적 치료 ! 조기에 항류마티스 약물 사용 단독보다 병합요법 단계적 약물 추가")
20
ACR treatment guideline for RA-use of biologics ACR guideline, Arthritis Rheum 2008 유병기간 6 개월 미만인 경우

21
Consensus statement on TNF blocking agent in JIA Etanercept(2 세이상 ), Adalimumab(4 세이상 ) Polyarticular type 유럽에서는 13-17 세 이상으로 승인 염증 조절되면 성장속도 회복에 기여
, Adalimumab(4 세이상 ) Polyarticular type 유럽에서는 세 이상으로 승인 염증 조절되면 성장속도 회복에 기여")
22
Etanercept ( Enbrel ) 적응증 : 투여법 : 보험적용 : 류마티스 관절염 (JIA 포함 ) 강직성 척추염, 건선관절염 25mg 1 주에 2 회 또는 50mg 1 주에 1 회 피하주사 항류마티스제를 사용해도 조절되지 않는 류마티스 관 절염, 강직성 척추염에서 보 험 적용. 자가주사 가능

23
*P < 0.05, combination vs MTX † P < 0.05, combination vs ETN *†*† *†*† Klareskog L, et al. Lancet. 2004;363:675-81. TEMPO Trial : 에타너셉트의 RA 관해 유도율 Patients in Remission (DAS44 <1.6)
.")
24
van der Heijde D, et al. 2004 *†*† *†*† 억제효과 개월 관절 손상 복구 가능성 TEMPO Trial: 에타너셉트의 방사선학적 진행 억제 (Disease Duration >3 yrs)
.")
25
Adalimumab (Humira) 자가로 맞을 수 있음 40mg s.c, 2 주에 1 회 적응증 : 류마티스 관절염 강직성 척추염, 건선관절염 크론병
 자가로 맞을 수 있음 40mg s.c, 2 주에 1 회 적응증 : 류마티스 관절염 강직성 척추염, 건선관절염 크론병")
26
Infliximab (Remicade) 적응증 : 류마티스 관절염 3mg/kg 크론씨병 강직성 척추염 5mg/kg 투여법 : Induction (0, 2, 6 주 ) IV 이후 6-8 주 간격으로 IV
 적응증 : 류마티스 관절염 3mg/kg 크론씨병 강직성 척추염 5mg/kg 투여법 : Induction (0, 2, 6 주 ) IV 이후 6-8 주 간격으로 IV")
27
Clinical Efficacy ……..All the same? DiseaseEtanerceptInfliximab Inflammatory Arthritis oo Heart Failure worsens ? worsens Crohn’s X o Clinical practice - switching may work Efficacy etanercept after failure infliximab mechanism ? lymphotoxin on biopsy (Buch et al ARD 2004;63(10):1344-6)
:1344-6).")
28
Consensus statement on TNF blocking agent in AS Indicated for active AS patients refractory to conventional Tx MTX, SSZ 과 병용가능하나 monoTx 보다 효과 좋다는 근거 없음 Etanercept, Adalimumab, Infliximab, Golimumab IBD 에 효과 - Adalimumab, Infliximab Onset time of action : within 6-12 주, 1 년까지 지연되기도. Recurrent uveitis, IBD 동반했을 때는 monoclonal Ab 제제가 선호됨

29
Example of Patient Pre- and Post-Treatment Gadolinium-enhanced T1 T9 T6 T2 T9 T6 T2 BaselineWeek 24

30
Improvement in MRI Activity Score at 24 Weeks Median Improvement (IQR)1 0.00 (-3.00, 0.57) 2.72 (-9.00, 0.00) Braun, et al. ACR 2004 late breaking abstract ASSERT: Infliximab in AS

31
* * * *P < 0.01 vs baseline After 24 weeks, PBO patients could switch to etanercept. Evaluated using T2-fat saturated MRI Baraliakos, et al. 2004; Poster presented at American College of Rheumatology, #L1. * Etanercept in AS: Effect on Spinal Inflammation

32
In RA First TNF blocker 에 non-responder 일 경우 second agent 에도 non-responder 일 가능성이 높으나 switching 으로 효과가 있을 수 있음 In A s 관찰연구에서 second agent 가 효과적일 수 있다는 결론 어느 것이 더 우수하다는 증거는 없음 Switching-TNF blocking agent

33
2006.10 Active ulcer was seen at the prox A-colon Azathioprine, Steroid, SSZ 2006. 12 bowel perforation F/39, 2005. 5 Behcet’s disease 진단

34
2009.10 복통 재발

35
After remicade induction (infusion 3 times)
")
36
여 /52, RA with persistent synovitis 2004. 2 월 RA 진단받음 PDL, Arava, Bredinin, SSZ, NMT, Cyclosporine 등 복용 MTX 는 intolerable 2007.09 Humira injection site reaction 으로 중단 2008.07 Enbrel 로 Switching 하여 start 3 개월 사용 후 ESR 43 16, CRP1.94 0.7

38
남 /39 AS with ulcerative colitis (UC) 2003.3 AS 진단 2005.1 UC 진단 Pentasa, PDL, SSZ, NSAID 복용 중에도 증상 지속 2007.11 Remicade 투여시작
 AS 진단 UC 진단 Pentasa, PDL, SSZ, NSAID 복용 중에도 증상 지속 Remicade 투여시작")
40
Demyelinating conditions Few reported cases among TNF-targeted agents : MS relapse, Paresthesia, Optic neuritis Some resolve spontaneously or upon discontinuation of Tx CHF Elevated TNF-a levels in patients with CHF associated with LV dysfunction Deleterious effects on LV remodeling Trials of TNF-targeted agents showed no benefit in CHF TNF 차단제의 문제점

41
ARTHRITIS & RHEUMATISM,60(7):1884–94, 2009 TNF 차단제의 문제점 - 결핵발생
:1884–94, 2009 TNF 차단제의 문제점 - 결핵발생")
42
결핵 발병율 차이 나는 이유 * 활성화된 macrophage 와 T cell 이 표현하는 mebrane bound TNF 가 결핵예방에 중요. 1) mAb 제제가 granuloma penetration 이 좋음 uveitis, Crohn’s disease 등의 granulomatous disease 에 mAb 가 더 effective 한 이유가 됨. 2) mAb 제제가 membrane bound TNF 에 대한 결합력이 좋아 apoptosis 더 잘 유발 3) mAb 제제가 LPS stimulated monocyte 의 IL-1 분비를 더 크게 방해
 mAb 제제가 granuloma penetration 이 좋음 uveitis, Crohn’s disease 등의 granulomatous disease 에 mAb 가 더 effective 한 이유가 됨. 2) mAb 제제가 membrane bound TNF 에 대한 결합력이 좋아 apoptosis 더 잘 유발 3) mAb 제제가 LPS stimulated monocyte 의 IL-1 분비를 더 크게 방해.")
43
양성 (10mm 이상 ) 최근 3 개월 결핵 접촉력 과거 치료력 무 / 부적절 과거 적절한 치료 없음 있음 조치 필요 없음잠복결핵 치료조치 필요 없음 현증 결핵 평가 피피디 검사 잠복결핵 대상자 선정 흐름표 흉부 엑스선 완치 흔적 흉부 엑스선 정상 임상적 증상 흉부 엑스선 이상 소견 흉부 엑스선 정상 흉부 엑스선, 임상적 평가 흉부 엑스선, 임상적 평가
 최근 3 개월 결핵 접촉력 과거 치료력 무 / 부적절 과거 적절한 치료 없음 있음 조치 필요 없음잠복결핵 치료조치 필요 없음 현증 결핵 평가 피피디 검사 잠복결핵 대상자 선정 흐름표 흉부 엑스선 완치 흔적 흉부 엑스선 정상 임상적 증상 흉부 엑스선 이상 소견 흉부 엑스선 정상 흉부 엑스선, 임상적 평가 흉부 엑스선, 임상적 평가")
44
잠복결핵의 치료 처방, 기간 및 용량 가. Isoniazid (INH), 9 개월 ( 최소 6 개월 ) - 용량은 5 (4 – 6) mg/kg, 최대 300 - 400mg/ 일 나. Rifampicin (RFP), 4 개월 - 용량은 10(8–12)mg/kg - BW 50kg 이상은 600mg/ 일, 그 미만은 450mg/ 일. 다. INH + RFP, 3 개월 라. RFP + pyrazinamide(PZA), 2 개월 - PZA 용량은 25(20–30)mg/kg, 일반적으로 1500mg/ 일, 2000mg/ 일을 초과하지 않도록. - 국외에서 중증의 간독성이 보고되었으므로 간질환이나 간독성의 위험인자가 있는 경우에는 사용하지 않는다. ※ 잠복결핵의 치료 3 주후부터 TNF 길항제의 투여를 시작하는 것이 바람직.
, 9 개월 ( 최소 6 개월 ) - 용량은 5 (4 – 6) mg/kg, 최대 mg/ 일 나. Rifampicin (RFP), 4 개월 - 용량은 10(8–12)mg/kg - BW 50kg 이상은 600mg/ 일, 그 미만은 450mg/ 일. 다. INH + RFP, 3 개월 라. RFP + pyrazinamide(PZA), 2 개월 - PZA 용량은 25(20–30)mg/kg, 일반적으로 1500mg/ 일, 2000mg/ 일을 초과하지 않도록. - 국외에서 중증의 간독성이 보고되었으므로 간질환이나 간독성의 위험인자가 있는 경우에는 사용하지 않는다. ※ 잠복결핵의 치료 3 주후부터 TNF 길항제의 투여를 시작하는 것이 바람직..")
45
Giant cell arteritis Takayasu’s arteritis Adult-onset Still’s disease Behçet’s disease Uveitis Sjögren’s syndrome Polymysositis Dermatomyositis SLE Systemic sclerosis Asthma IPF Additional possible indications for TNF- targeted biologic Tx Furst DE, et al. Ann Rheum Dis. 2004;63(S2): ii1-ii12.
: ii1-ii12..")
46
IL-1 inhibitor

47
Anakinra (Kineret ® ) No signalling Anakinra IL-1 IL-1Ra recombinant human form of the naturally occurring IL-1 receptor antagonist Indication: - RA (A) - systemic type JIA (D) - Adult onset Still’s disease (D)
 No signalling Anakinra IL-1 IL-1Ra recombinant human form of the naturally occurring IL-1 receptor antagonist Indication: - RA (A) - systemic type JIA (D) - Adult onset Still’s disease (D)")
48
Nancy J. Olsen NEJM 2004;350:2167-79. Rate of reponse of anakinra

49
Rilonacept in gouty arthritis Ann Rheum Dis 2009;68;1517-19 Rilonacept: soluble receptor-Fc fusion protein engages and inhibits IL-1

50
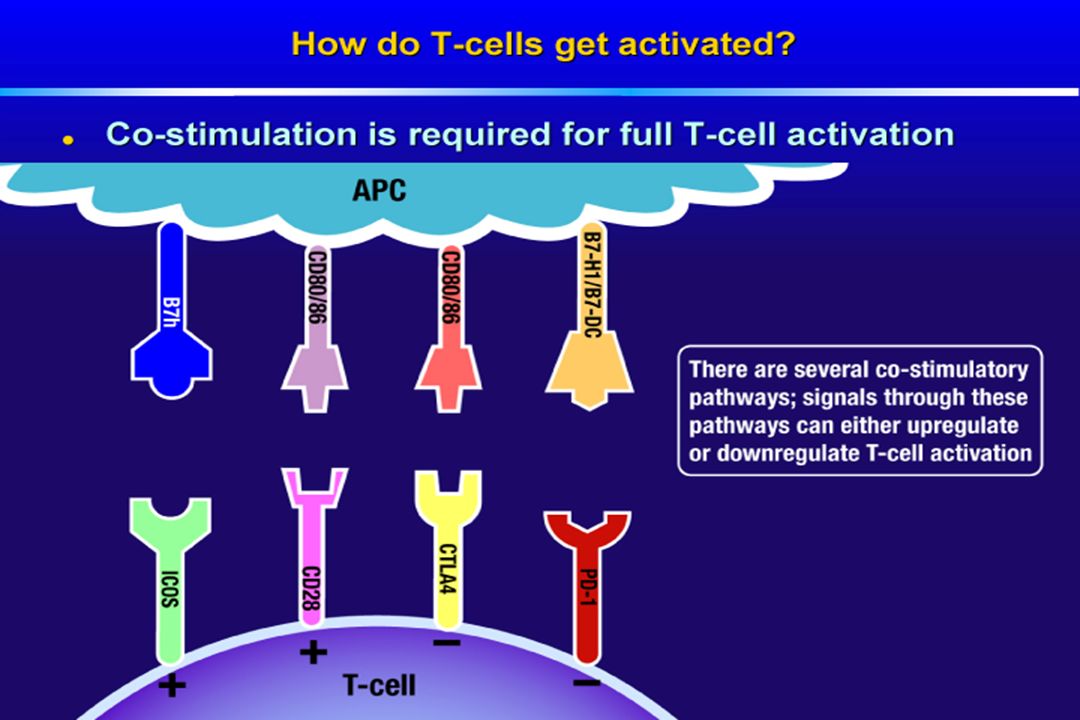
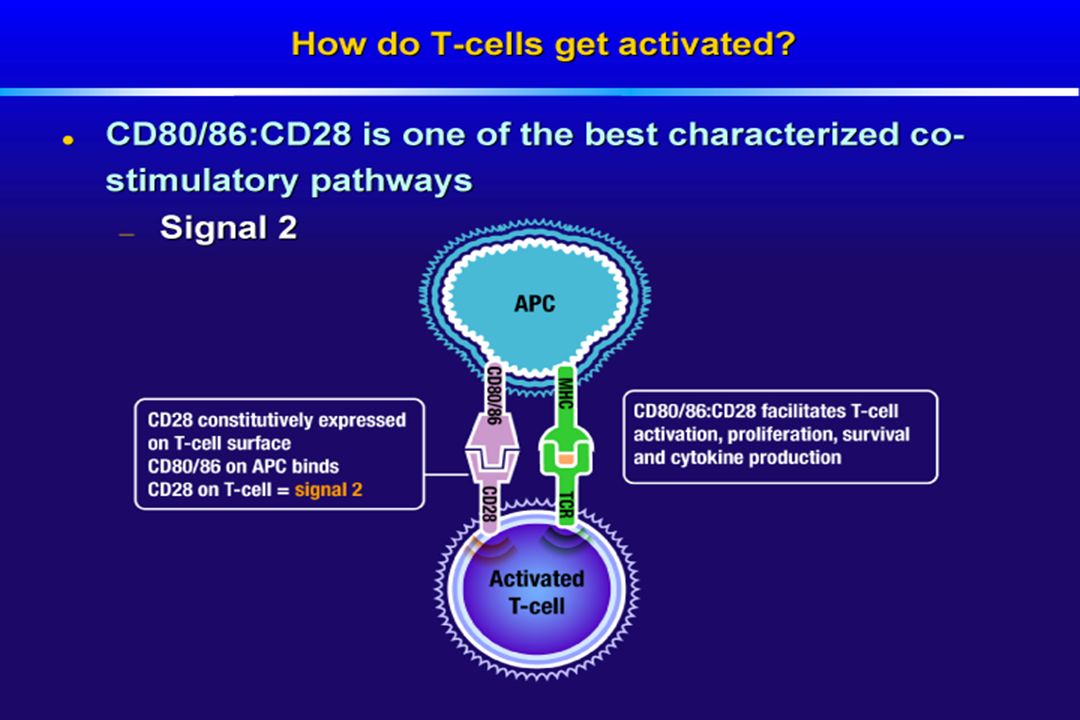
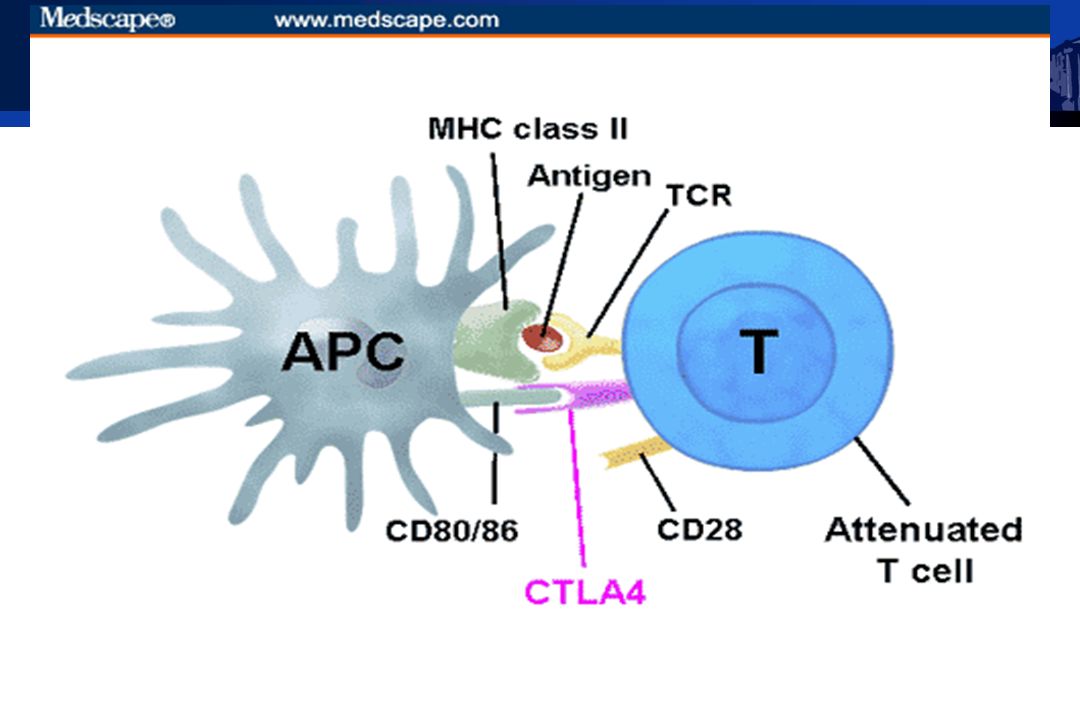
Costimulatory molecule inhibition

54
Abatacept (Orencia) Cell membrane Cytotoxic T lymphocyte-associated antigen 4 (CTLA) External Internal IgG1 CTLA4-Ig : an Immunoglobulin fusion protein
 Cell membrane Cytotoxic T lymphocyte-associated antigen 4 (CTLA) External Internal IgG1 CTLA4-Ig : an Immunoglobulin fusion protein")
55
Effects of fusion protein CTLA4Ig : for RA patients refractory to MTX Joel M. Kremer, NEJM 2003;349:1907-15

56
Abatacept for RA refractory to TNF-α Inhibition Mark C. Genovese, NEJM 2005;353:1114-23

57
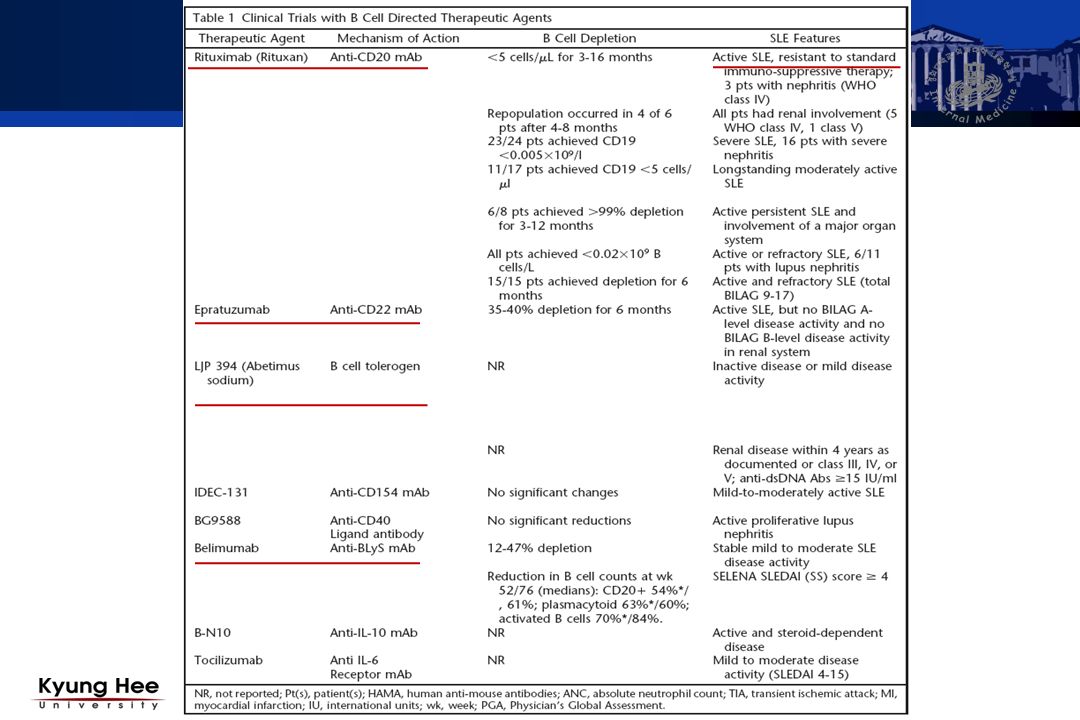
B cell depletion Tx

58
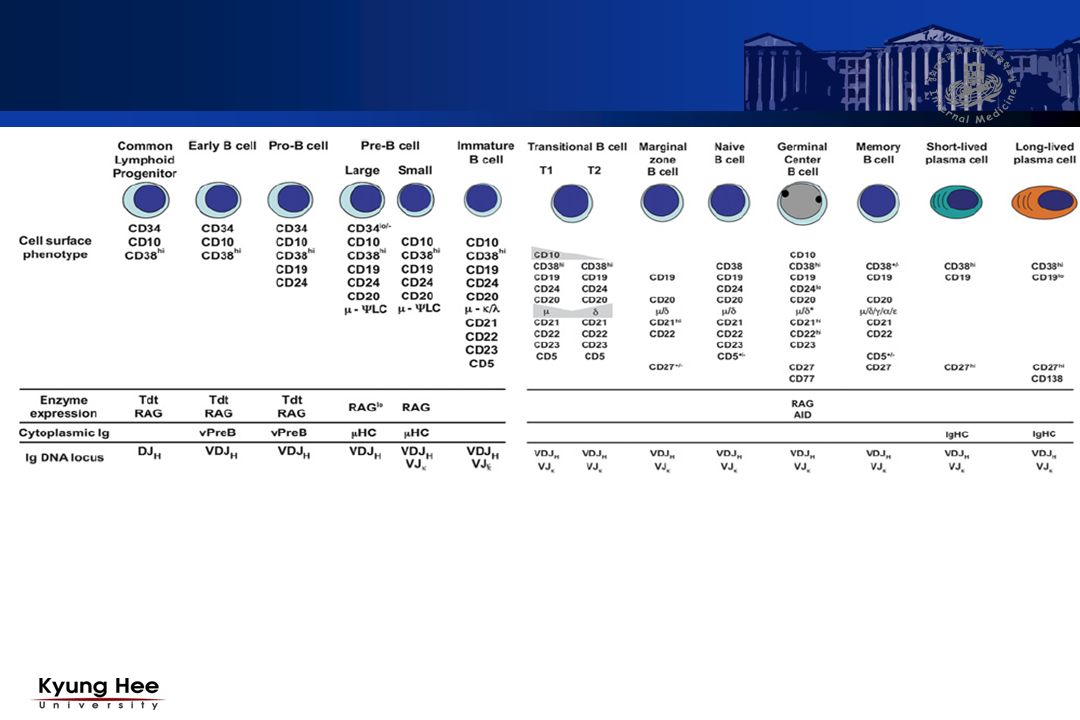
B cell surface antigen

59
Rituximab (Mabthera ® )
")
60
B cells depeletion in RA Tx Potential roles of B cells AutoAb production Ag presentation Co-stimulation Cytokine production Chemokine production CD20: B-cell surface antigen Rituximab: anti-CD20 monoclonal Ab Relapsed or refractory low grade or follicular CD20+ B cell NHL Causes selective transient depletion of CD 20 + B cell subpopulation

62
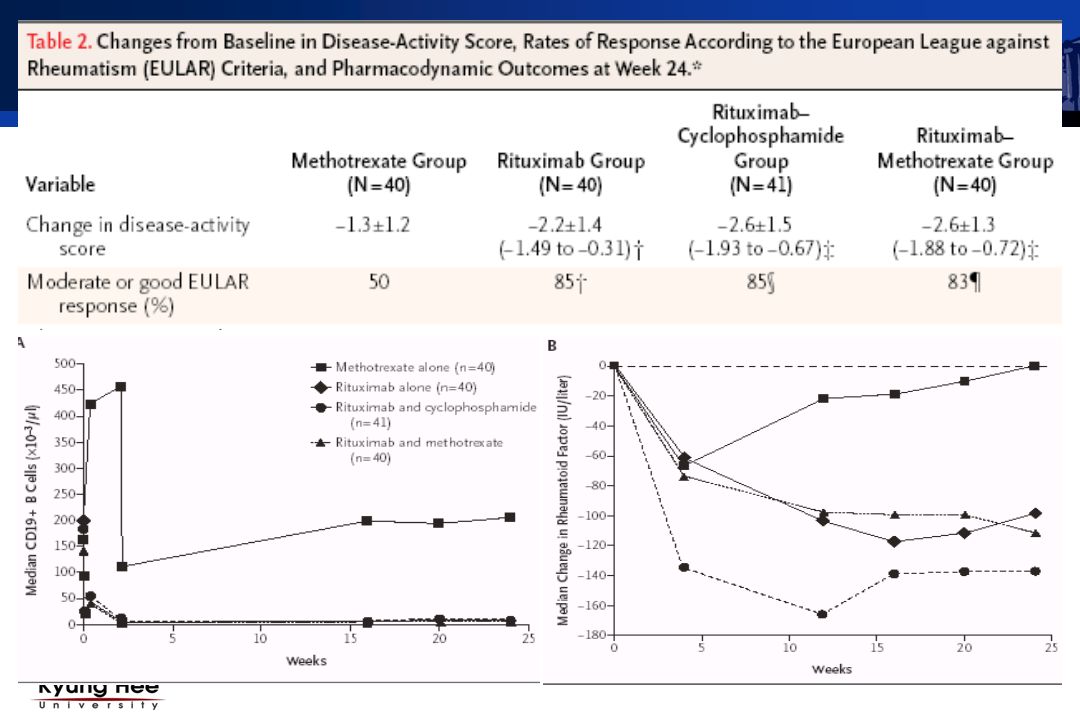
Rituximab for RA : Study protocol Active seropositive RA despite MTX use at least 10mg/week, > 16 week 1. Control: oral MTX 10mg or more / week plus placebo 2. Rituximab + placebo for MTX and cyclophsphamide 3. Rituximab + cyclophsphamide in IV 750mg on 3,17 + placebo for MTX 4. Rituximab + MTX + placebo for cyclophsphamide MPD 1000mg 2 주간격으로 두번 IV +PDL 60mg, 30mg

64
The American Journal of Geriatric Pharmacotherapy Vol.5 (3) Sep 2007 Indications for Rituximab
 Sep 2007 Indications for Rituximab")
66
Conclusion Biologic agents : important advance in the treatment of rheumatic diseases TNF-targeted biologics : some of the challenges in the treatment of rheumatic diseases TNF-targeted biologics: established, long-term efficacy across several indications : RA, AS, PsA, Other conditions (eg, Crohn’s) Use expanding to additional diseases/indications
 Use expanding to additional diseases/indications")
Similar presentations

, PR(+) –HER-2: +3.>")



 주요 내용 소개>")


![MGR review 류마티스 내과 R4 최인아. [ 목차 ] Overlap syndrome (vs UCTD, MCTD) Polymyositis(PM) PM with Interstitial lung disease.](/42/11353284/big_thumb.jpg "MGR review 류마티스 내과 R4 최인아. [ 목차 ] Overlap syndrome (vs UCTD, MCTD) Polymyositis(PM) PM with Interstitial lung disease.>")
 비만률순위 : 29 위 (2005 OECD)>")

>")





- Agonists against Hepatitis B virus (HBV)-associated Hepatocellular.>")

