Download presentation
Presentation is loading. Please wait.

1
Case Presentation Thoracic and Cardiovascular surgery department, SMC
Son Eui Young 1

2
Chief Complaint M / 2개월 11일 Abnormal echocardiography result
Onset : Page 2

3
Present illness 2개월 남아, 31+0wk, 1.69kg, syphilis mother's baby, C/sec d/t PPROM and breech presentation, Apgar score 2/2으로 출생 출산 후 시행한 TTE 상 VSD 및 ASD 소견 관찰 이에 대해 further evaluation 및 management 위하여 본원 NICU 전원 Page 3

4
Other Histories Development: normal Surgical history: none
Current medication: none 과거력상 특이 소견 없었습니다. Page 4

5
Review of System 특이사항 없음 General Weakness(-)
Fever/Chill/Night sweat(-/-/-) Headache/Dizziness(-/-) Visual disturbance/ocular pain(-/-) Sore throat/Rhinorrhea/Sneezing(-/-/-) Cough/Sputum (-/-/-) Dyspnea/Hemoptysis (-/-) Chest pain (-) Palpitation (-) Abdominal pain (-) Anorexia/Nausea/Vomiting(-/-/-) Constipation/Diarrhea(-/-) Melena/hematochezia/ hematemesis (-/-/-) Dysuria/Frequent voiding(-/-) Red urine/Foamy urine(-/-) Arthralgia/Myalgia (-/-) Morning stiffness(-/-/-) Easily bruisilibility (-) ROS 상에서는 원래 가지고 있던 n/v의외에 다른 증상은 없었습니다. Page 5
 Headache/Dizziness(-/-) Visual disturbance/ocular pain(-/-) Sore throat/Rhinorrhea/Sneezing(-/-/-) Cough/Sputum (-/-/-) Dyspnea/Hemoptysis (-/-) Chest pain (-) Palpitation (-) Abdominal pain (-) Anorexia/Nausea/Vomiting(-/-/-) Constipation/Diarrhea(-/-) Melena/hematochezia/ hematemesis (-/-/-) Dysuria/Frequent voiding(-/-) Red urine/Foamy urine(-/-) Arthralgia/Myalgia (-/-) Morning stiffness(-/-/-) Easily bruisilibility (-) ROS 상에서는 원래 가지고 있던 n/v의외에 다른 증상은 없었습니다. Page 5.")
6
Physical Exam Vital sign General appearance: Acute ill-looking
BP 110/70, HR 94, RR 16, BT 36.3℃ SpO2 94% General appearance: Acute ill-looking Mental state: alert & well oriented GCS (E 4, V 5, M 6) Head and Neck Pinkish Conjunctiva/ unicteric Sclera Isocoric Pupil size, prompt light reflex at both eyes Nystagmus ( - ) Otoscopy (정상) oral ulcer ( - ), tongue dehydration ( - ) Tonsilar hypertrophy( - ), Pharyngeal injection( - ) Cervical LNE( -); Thyroid enlargement ( - ) Carotid bruit Rt/Lt ( - / - ) Paranasal tenderness ( - ) Chest Symmetric expansion chest wall retraction (+) : subcostal Vesicular Breath sound s wheezing Murmur (+) Lower Left sternal border, pansystolic grade 3 Subclavicular node / Axillary node ( - / - ) Abdomen Liver palpation( - ) Spleen palpation ( - ) Skin Rash/Purpura/erythema (- / - / - ) 피지컬 상에서 vital sign은 비교적 안정적이었고 급성병색이었으며 심장음과 호흡음에서 이상음은 들리지 않았습니다. Page 6
 Head and Neck. Pinkish Conjunctiva/ unicteric Sclera. Isocoric Pupil size, prompt light reflex at both eyes. Nystagmus ( - ) Otoscopy (정상) oral ulcer ( - ), tongue dehydration ( - ) Tonsilar hypertrophy( - ), Pharyngeal injection( - ) Cervical LNE( -); Thyroid enlargement ( - ) Carotid bruit Rt/Lt ( - / - ) Paranasal tenderness ( - ) Chest. Symmetric expansion. chest wall retraction (+) : subcostal. Vesicular Breath sound s wheezing. Murmur (+) Lower Left sternal border, pansystolic grade 3. Subclavicular node / Axillary node ( - / - ) Abdomen. Liver palpation( - ) Spleen palpation ( - ) Skin. Rash/Purpura/erythema (- / - / - ) 피지컬 상에서 vital sign은 비교적 안정적이었고. 급성병색이었으며. 심장음과 호흡음에서 이상음은 들리지 않았습니다. Page 6.")
7
Page 7

8
Echocardiogram , #18 1) Large PMOE VSD (9.6mm) with left-to-right dominant bidirectional shung 2) Large secundum ASD (8.8 x 7.4 mm) with left-to-right shunt 3) dilated RA & RV 4) no PDA, no CoA 그래서 그라목손의 acute intoxication impression 하에 Page 8
 Large secundum ASD (8.8 x 7.4 mm) with left-to-right shunt. 3) dilated RA & RV. 4) no PDA, no CoA. 그래서 그라목손의 acute intoxication impression 하에. Page 8.")
9
Initial Lab 그래서 그라목손의 acute intoxication impression 하에 Page 9

10
Problem List #1. Preterm AGA #2. Low birth weight infant
#3. Syphilis mother's baby #4. Abnormal echocardiographic finding including VSD 그래서 그라목손의 acute intoxication impression 하에 Page 10

11
Assessment #1, #2, #4 VSD (SA, small to moderate)
그래서 그라목손의 acute intoxication impression 하에 Page 11

12
Plan VSD closure with bovine pericardium ASD primary closure Page 12

13
Operation Operation 수술 후 진단명 VSD closure with bovine pericardium
ASD primary closure 수술 후 진단명 VSD (PMOE, large) ASD (secundum, large) 환자 입원 후 높은 사망가능성 및 예후가 안 좋음을 설명하였고, hydration 과 dexamethasone 그리고 hemoperfusion을 시행해주었습니다. 기본 랩들과 chest AP를 찍었스빈다. Page 13
 ASD (secundum, large) 환자 입원 후 높은 사망가능성 및 예후가 안 좋음을 설명하였고, hydration 과 dexamethasone 그리고 hemoperfusion을 시행해주었습니다. 기본 랩들과 chest AP를 찍었스빈다. Page 13.")
14
Page 14

15
Hospital Course – POD #1 응급실 입원 1일 째, 다른 문제는 없었으나 cost문제로 결국 타 병원으로 이송되었습니다. Page 15

16
Ventricular Septal Defect 2007313075 Son Eui Young
Disease Review 디지즈 리뷰에서는 그라목손이 속한 쿼터너리 나이트로겐 컴파운드 계열의 drug intoxication에 대해서 말씀드리겠습니다. Ventricular Septal Defect Son Eui Young 16

17
Introduction 1 in 1000 live births 선천성 심질환 중 가장 흔하다. (단독으로는 25%)
50% associated with other congenital malformations First described by Roger in 1879, hence small VSDs are also known as the ‘maladie de Roger’. First VSD closed under direct vision by Lillehei in 1955 태어나는 아기 1000명중 1명 꼴로 발생하는, 선천성심질환 중 가장 흔한 병입니다. 단독으로는 25%정도이며, VSD중 절반은 다른 기형을 동반합니다. 라거~라는 사람이 처음 describe 하였고, 릴레이~라는 사람이 처음으로 VSD를 닫았다고 합니다. Page 17

18
Anatomic Classification of VSD
Perimembranous: 80% Subarterial: 14% Muscular VSD : 10% Figure 117–4 Classification of ventricular septal defects (VSDs):
:")
19
Commonly Associated Defects
Patent ductus arteriosus (PDA) :25% Diagnostic difficulties:preop.echo, TEE etc should be ligated or clipped Coarctation or Aorta : 10% Augmented L-R shunt left ventricular outflow tract obstruction(Congenital valvar or subvalvar aortic stenosis): 4% large atrial septal defects (ASDs), right ventricular outflow tract obstruction, vascular ring, and persistent left superior vena cava.
 :25% Diagnostic difficulties:preop.echo, TEE etc. should be ligated or clipped. Coarctation or Aorta : 10% Augmented L-R shunt. left ventricular outflow tract obstruction(Congenital valvar or subvalvar aortic stenosis): 4% large atrial septal defects (ASDs), right ventricular outflow tract obstruction, vascular ring, and persistent left superior vena cava.")
20
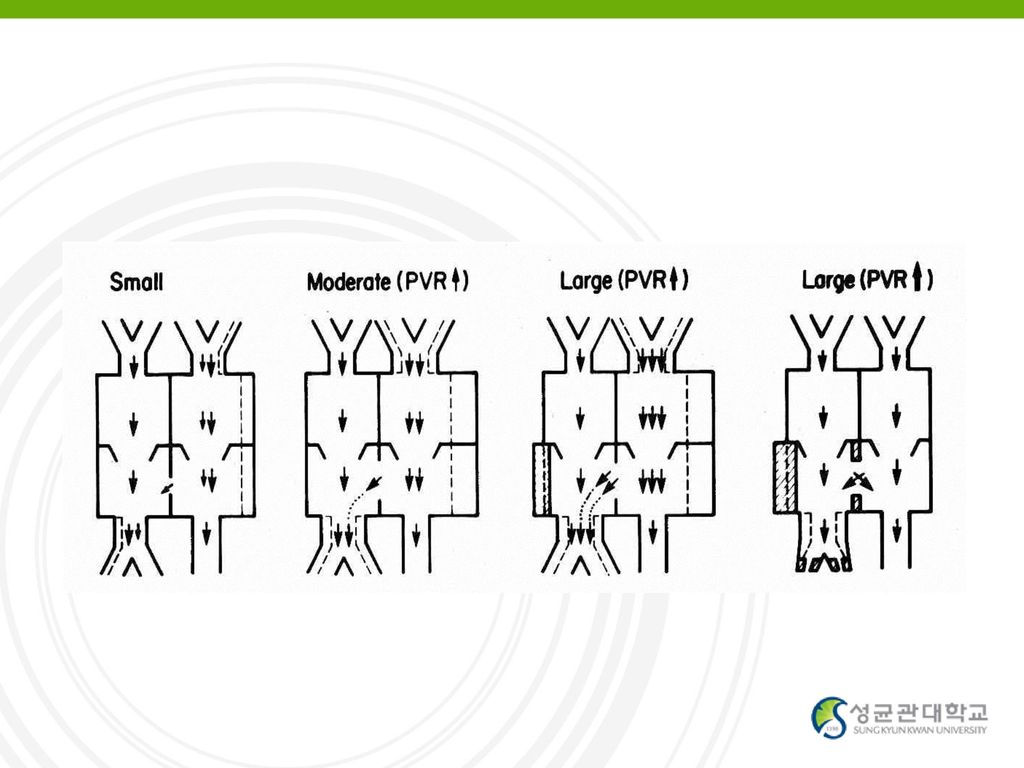
Pathophysiology Shunt Direction and Magnitude Small size
depend on the size of the defect and the pressure gradient Qp/Qs Small size RV의 수축기압을 의미있게 증가시키지 못하는 작은 결손 폐동맥혈류 증가가 심하지 않음 (Qp/Qs < 1.75) 폐동맥고혈압 없음 Large size : 결손 크기가 aortic valve ring 보다 클 때 폐혈관저항 증가 (Qp/Qs > 2) 우심실과 좌심실간의 압력차가 소실되거나 역전되어 L-R shunt와 R-L shunt 가 같이 생김 청색증, 객혈, 심부전증 등이 나타나 사망할 수 있음 병태생리는 크기에 따라 결정됩니다.
 폐동맥고혈압 없음. Large size : 결손 크기가 aortic valve ring 보다 클 때. 폐혈관저항 증가 (Qp/Qs > 2) 우심실과 좌심실간의 압력차가 소실되거나 역전되어 L-R shunt와 R-L shunt 가 같이 생김. 청색증, 객혈, 심부전증 등이 나타나 사망할 수 있음. 병태생리는 크기에 따라 결정됩니다.")
22
Complication Growth failure
Congestive heart failure (left heart failure) Pulmonary vascular disease :as Eisenmenger syndrome or complex Severe illness with viral or bacterial pneumonia Infective endocarditis Aortic regurgitation Stenosis in the right ventricular outflow tract Discrete fibrous subaortic stenosis Acquired left ventricular outflow tract obstruction Aneurysm of the ventricular septum Paradoxical emboli Sudden death Heart block secondary to intracardiac repair Impaired left ventricular function in some patients Increase in weight following VSD closure
 Pulmonary vascular disease :as Eisenmenger syndrome or complex. Severe illness with viral or bacterial pneumonia. Infective endocarditis. Aortic regurgitation. Stenosis in the right ventricular outflow tract. Discrete fibrous subaortic stenosis. Acquired left ventricular outflow tract obstruction. Aneurysm of the ventricular septum. Paradoxical emboli. Sudden death. Heart block secondary to intracardiac repair. Impaired left ventricular function in some patients. Increase in weight following VSD closure.")
23
Diagnostic work-up Symptoms
tachypnea, growth failure, profuse sweating during feeding, a bulging precordium, a pansystolic murmur, an enlarged liver, and thready pulses the physical examination, chest radiograph, and electrocardiogram (ECG)
")
24
VSD Natural Course Spontaneous closure or decrease of size
Perimembranous or muscular type Aggressive medical management cf. Malalignment type, SA, MO, Endocardial cushion type Usually within 6-12 Mo of age

25
VSD Natural Course Eisenmenger or Severe PHT
Usually after 1 yr of age Contraindications for op d/t PHT - PVR > 8-10 Wood unit - No response to pulmonary vasodilators such as O2 or nitric oxide - Mainly R-L shunt or no L-R shunt through VSD

26
VSD Natural Course AV Deformity
Mainly subarterial type Some of PM type MO VSD Increased incidence of infective endocarditis if there is AR

27
VSD Natural Course Subaortic stenosis
Usually discrete membrane type Occasionally tunnel type Op indications AV deformity PG > mm Hg

28
Treatment of VSD : Indications
Approximately 30% of infants surgery within the first year of life Significant shunt Medically uncontrolled CHF PA pressure > 1/2 of systemic artery pressure Shunt amount; Qp/Qs > 1.5 or 1.7 Other problems DCRV, Subaortic stenosis, AV deformity Consider natural course, patient’s age

29
Treatment of VSD : depends on size
Large VSD < 3 months – CHF, failure to thrive Elective repair at 6-12 months (PVR < 8.0 units) Small VSD (Qp:Qs<2:1) Endocarditis Cardiac Enlargement Any Aortic Incompetence Subarterial (supracristal) VSD - any size, operate early
 Small VSD (Qp:Qs<2:1) Endocarditis. Cardiac Enlargement. Any Aortic Incompetence. Subarterial (supracristal) VSD - any size, operate early.")
Similar presentations






 3 days ago CC: Feveronset) 3 days ago PI : F/29, 5 년전 첫아기 임신 8 개월째에.>")

 주요 내용 소개>")




 C.C. > Anorexia o/s) 내원 약 4 주전 P. I. > 1 년 간 7kg 의 weight loss 있었고, 두 달 전 시행한 abd CT 및 위내시경에서 양성종양 발견되어 observation 하던 중, 최 근 한 달.>")





