Download presentation
1
Department of Hemato-oncology Hematopoietic Cell Transplantation FROM UNRELATED DONORS

2
Contents History Allogenic HCT From Unrelated donor Reduced Intensity Conditioning Regimen GVHD

3
History 1958 년 프랑스 Jean Dausset human histocompatibility antigens HLA 가 완전히 일치하는 일란성 쌍둥이간의 골수 이식 형제간의 골수 이식 1968 년 University of Minnesota severe combined immunodeficiency disease, 소아 비혈연간 골수이식 1973. Memorial Sloan-Kettering Cancer Center severe combined immunodeficiency disease Denmark 혈액 은행을 통해 발견한 기증자의 골수 이식

4
각국의 골수기증희망자 등록기관 WMDA(World Marrow Donor Association) 타국의 비혈연 환자들 국제적인 비영리조직. 2001 년 12 월말 현재 7,435,301 명 미국, NMDP(National Marrow Donor Program) 1987 년 연방정부의 위탁 독립적인 The American Bone Marrow Donor Registry 일본의 JMDP(Japan Marrow Donor Program)
 1987 년 연방정부의 위탁 독립적인 The American Bone Marrow Donor Registry 일본의 JMDP(Japan Marrow Donor Program).")
5
국가별 골수기증희망자 등록 ( 모집 ) 현황 국가미국독일일본한국 골수기증 희망등록자 3476615160585913893252204 총인구수 2783570008222000012671400047275000 인구대비 1.25%1.95%0.12%0.11%
 현황 국가미국독일일본한국 골수기증 희망등록자 총인구수 인구대비 1.25%1.95%0.12%0.11%")
6
Annual Number of HCT Worldwide NUMBER OF TRANSPLANTS YEAR 197019751980198519901995 0 5,000 10,000 15,000 20,000 25,000 30,000 35,000 40,000 Autologous Allogeneic 2000 (IBMTR)
")
7
Indications for HCT in North America TRANSPLANTS 4,500 0 500 1,000 1,500 2,000 Non-Hodgkin Lymphoma AMLCMLHodgkin Disease Ovarian Cancer Allogeneic (Total N = 6,700) Autologous (Total N = 11,000) 2,500 3,000 4,000 3,500 Multiple Myeloma Breast Cancer ALLMDS/Other Leukemia Other Cancer Non-Malignant Disease CLL (IBMTR, year 2000)
 Autologous (Total N = 11,000) 2,500 3,000 4,000 3,500 Multiple Myeloma Breast Cancer ALLMDS/Other Leukemia Other Cancer Non-Malignant Disease CLL (IBMTR, year 2000)")
8
Availability of Different Types of Donor Chance of finding a donor (%) Related genotypic match Unrelated phenotypic match Related genotypic haplo-identical Partial Mismatch 6 / 6 5 - 6 / 6 4 / 6 3 / 6
 Related genotypic match Unrelated phenotypic match Related genotypic haplo-identical Partial Mismatch 6 / / 6 4 / 6 3 / 6")
9
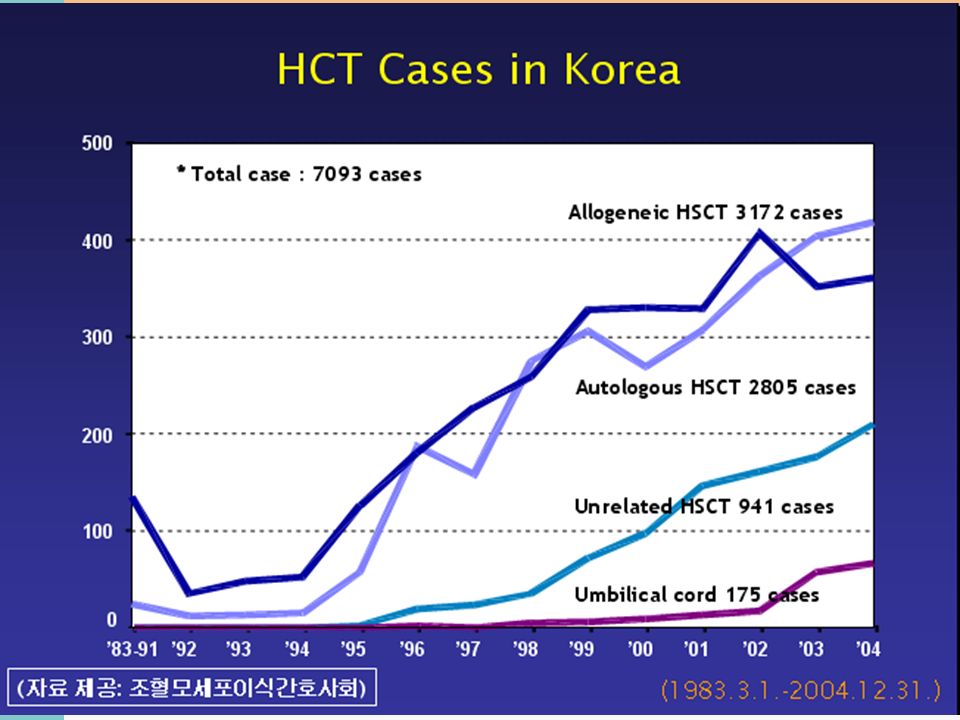
우리나라의 비혈연조혈모세포기증 사업 1993 년 3 월. 사랑의장기기증운동본부에서 사랑의골수은행 설립 한국조혈모세포은행 정부 위탁 대한적십자사 및 사랑의장기기증운 국내 모든 의료기관의 환자들에게 이식을 지원, 조정 민간 - 가톨릭골수정보은행 가톨릭조혈모세포은행에서만 활용

11
BMT 의 목적 재생불량성빈혈 또는 중중복합면역부전증에서와 같이 양적 혹은 질 적으로 이상이 있는 환자의 조혈모세포를 골수 공여자의 정상 조혈 모세포로 바꾸어 넣어 정상 조혈모세포 유래의 세포로 재구축을 하 는 조혈모세포의 보충 목적. 백혈병 등에서와 같이 치사량의 전신 방사선 조사나 초대량의 화학 요법으로 백혈병세포를 섬멸시키고 이로 인하여 황폐화된 골수를 골수공여자 ( 혹은 미리 채취한 자가 골수 내지는 말초혈액 ) 유래의 정상 조혈모세포로 바꾸어 넣는 목적.
 유래의 정상 조혈모세포로 바꾸어 넣는 목적..")
13
Hematopoietic Cell Transplantation Donor sources Autologous Non-autologous syngeneic allogeneic - sibling, family member, unrelated Hematopoietic graft sources Bone marrow Peripheral blood Umbilical cord

14
Donor Selection in Allogeneic BMT Immunogenic relationship between donor and recipient Graft rejection GVHD GVT (graft-versus-tumor) effect Possible stem cell donors HLA-genotypically matching sibling donor HLA-haploidentical family member (with limited disparity) HLA-phenotypically identical unrelated donor
 effect Possible stem cell donors HLA-genotypically matching sibling donor HLA-haploidentical family member (with limited disparity) HLA-phenotypically identical unrelated donor")
15
Allogenic HCT GVHD, rejection Major antigen – HLA mismatched Minor antigen – endogenous proteins 1.5~5 * 10 8 nucleated BM cell/kg Survival following one Ag mismatched transplant is not remarkablly altered Transplantation of higher number of BM cell - improved survival

16
a marrow cell dose above 3.5* 10 8 /kg, and cytomegalovirus seronegative status before BMT in both patient and donor were favorable prognostic factors. a high marrow cell dose and improved survival and support the use of unrelated donor BMT for treatment of patients with high risk AML when a family match is not available. Bone Marrow Transplantation (2000) 26, 397–404.
 26, 397–404..")
17
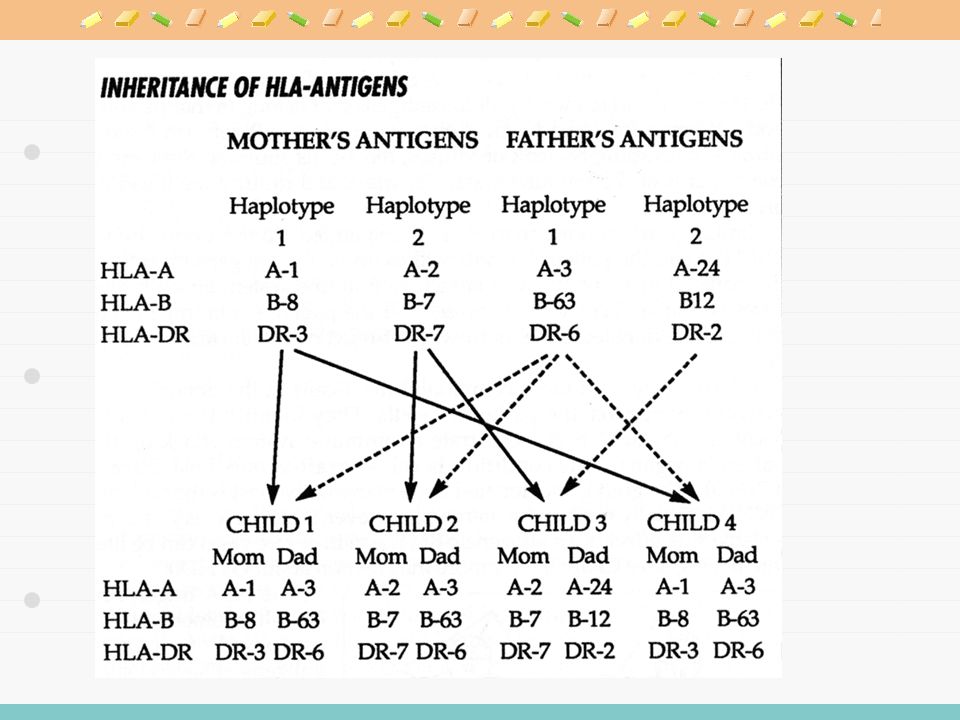
HLA (Human Leukocyte Antigens) HLA-class I Single polymorphic -chain + 2-microglobulin HLA-A (85 alleles), B (188 alleles), C (42 alleles) Allo-response: HLA-A, B, C genes HLA-class II Polymorphic (DQ, DP) or non-polymorphic (DR) -chain + polymorphic -chain -chain: DRA, DQA (18 alleles), DPA -chain: DRB (B1 [220 alleles], B3, B4, B5), DQB (31 alleles), DPB Allo-response: HLA-DRB1, DQ genes * Human MHC in chromosome 6, short arm * Minor histocompatibility antigens
![HLA (Human Leukocyte Antigens) HLA-class I Single polymorphic -chain + 2-microglobulin HLA-A (85 alleles), B (188 alleles), C (42 alleles) Allo-response: HLA-A, B, C genes HLA-class II Polymorphic (DQ, DP) or non-polymorphic (DR) -chain + polymorphic -chain -chain: DRA, DQA (18 alleles), DPA -chain: DRB (B1 [220 alleles], B3, B4, B5), DQB (31 alleles), DPB Allo-response: HLA-DRB1, DQ genes * Human MHC in chromosome 6, short arm * Minor histocompatibility antigens](http://images.slidesplayer.org/39/10970403/slides/slide_17.jpg "HLA (Human Leukocyte Antigens) HLA-class I Single polymorphic -chain + 2-microglobulin HLA-A (85 alleles), B (188 alleles), C (42 alleles) Allo-response: HLA-A, B, C genes HLA-class II Polymorphic (DQ, DP) or non-polymorphic (DR) -chain + polymorphic -chain -chain: DRA, DQA (18 alleles), DPA -chain: DRB (B1 [220 alleles], B3, B4, B5), DQB (31 alleles), DPB Allo-response: HLA-DRB1, DQ genes * Human MHC in chromosome 6, short arm * Minor histocompatibility antigens")
20
Age or comorbid conditions Reduced intensity conditioning regimens Donor availability Marrow donor program Cord blood transplantation Haplo-identical HCT Post-transplant complications Engraftment failure Non-relapse mortality & morbidity Relapse of underlying disease Limitations of Allogeneic HCT

21
Complications of Allogeneic BMT RRT Bleeding Bacterial and fungal infections VOD H. simplex Acute GVHD Chronic GVHD IP, CMV, PCP Varicella zoster -702149100365

22
HCT from unrelated donor Cure for hematologic malignancy HLA system, MHC HLA-typed volunteer donor Unrelated donor HCT-improved HVG and GVH reaction Less toxic transplant regimen Prevention and treatment of GVHD Supportive care of the transplant recipient

23
Conditioning Regimens Purpose Marrow space for donor stem cells (marrow ablation) Suppression of the recipient’s immune system Eradication of malignant or abnormal cell population Common regimens Leukemia, MDS: cytoxan + TBI, busulfan + cytoxan Aplastic anemia: cytoxan + ATG Reduced intensity conditioning regimen
 Suppression of the recipient’s immune system Eradication of malignant or abnormal cell population Common regimens Leukemia, MDS: cytoxan + TBI, busulfan + cytoxan Aplastic anemia: cytoxan + ATG Reduced intensity conditioning regimen")
24
Characteristics of reduced intensity conditioning (RIC) regimen Reversible myelosuppression (usually within 28 days) without stem cell support Mixed chimerism in a proportion of patients at the time of first assessment Low rates of non-hematologic toxicity Definitions of RIC regimens by CIBMTR & NMDP ≤ 500 cGy TBI ≤ 9 mg/kg total busulfan dose ≤ 140 mg/m 2 total melphalan dose ≤ 10 mg/kg total thiotepa dose Usually includes a purine analog – fludarabine, cladribine, or pentostatin Reduced Intensity Conditioning Regimen
 regimen Reversible myelosuppression (usually within 28 days) without stem cell support Mixed chimerism in a proportion of patients at the time of first assessment Low rates of non-hematologic toxicity Definitions of RIC regimens by CIBMTR & NMDP ≤ 500 cGy TBI ≤ 9 mg/kg total busulfan dose ≤ 140 mg/m 2 total melphalan dose ≤ 10 mg/kg total thiotepa dose Usually includes a purine analog – fludarabine, cladribine, or pentostatin Reduced Intensity Conditioning Regimen")
25
Most commonly used RIC regimens as reported to the CIBMTR by ascending myelosuppressive intensity Fludarabine ± others : 10% Fludarabine/TBI ± others : 31% Fludarabine/cyclophosphamide ± others : 17% Fludarabine/busulfan ± others : 27% Fludarabine/melphalan ± others : 15% Reduced Intensity Conditioning Regimen

26
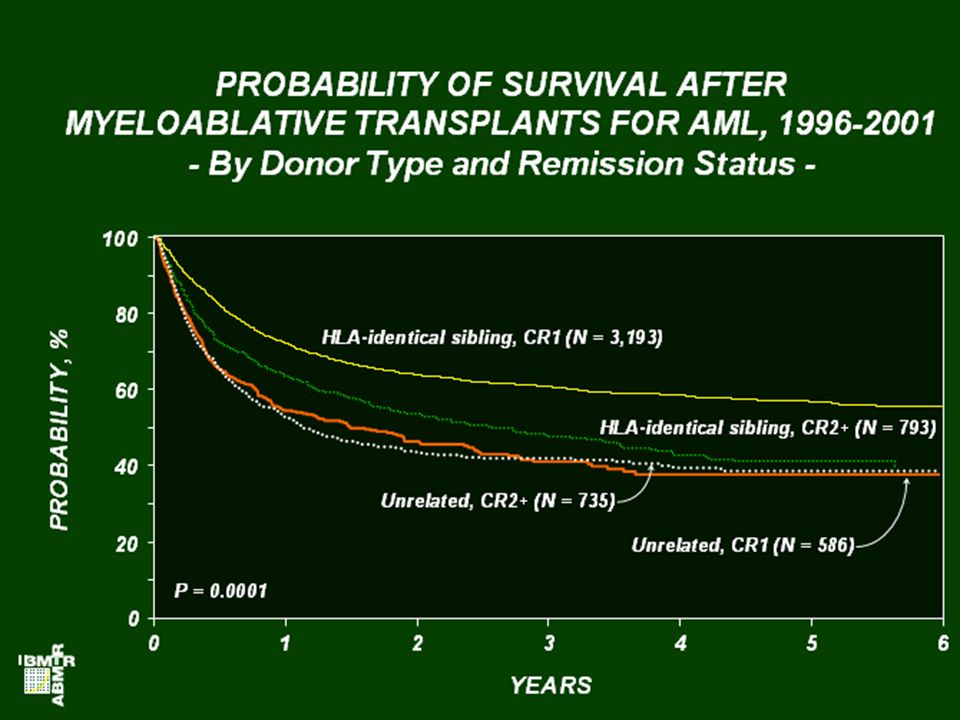
BMT from Unrelated donor Outcomes are improving similar - matched sibling allografts Role of UD-SCT closeness of HLA matching age of the patient CMV serostatus of recipient and donor

27
BMT from Unrelated donor Recent developments peripheral blood stem cells from unrelated donors PCR to diagnose CMV and fungal infections reduced intensity conditioning A matched sibling donor preferable to an unrelated donor graft-versus- tumour effect, though In second complete remission, UD-SCT Antecedent myelodysplasia Cytogenetic abnormalities persist

28
Evidence of GVL Effects (1) Temporal associations between GVHD and hematological remission (2) Incidence of leukemic relapse is lower after allogeneic BMT than after syngeneic BMT. (3) Incidence of leukemic relapse is lower in allogeneic marrow recipients in whom GVHD develops than in allogeneic marrow recipients in whom GVHD does not develop. (4) Incidence of leukemic relapse is lower in recipients of allogeneic marrow without GHVD than in recipients of syngeneic marrow. (5) Incidence of leukemic relapse is higher in recipients of T-cell-depleted allogeneic marrow than in recipients of unmodified allogeneic marrow. (6) Infusions of donor lymphocytes can reinduce remissions in many patients who have CML, CLL, myeloma, and lymphoma relapsing after allogeneic BMT.
 Incidence of leukemic relapse is lower in allogeneic marrow recipients in whom GVHD develops than in allogeneic marrow recipients in whom GVHD does not develop. (4) Incidence of leukemic relapse is lower in recipients of allogeneic marrow without GHVD than in recipients of syngeneic marrow. (5) Incidence of leukemic relapse is higher in recipients of T-cell-depleted allogeneic marrow than in recipients of unmodified allogeneic marrow. (6) Infusions of donor lymphocytes can reinduce remissions in many patients who have CML, CLL, myeloma, and lymphoma relapsing after allogeneic BMT..")
29
GVHD vs. Relapse

30
CR2 in AML Which type of transplant is better? Auto or Allo? best treated by UD-SCT Young patients with a 10-antigen matched donor adverse cytogenetics short first remissions Autologous SCT and a much lower TRM >40 years long first remissions UD-HCT in AML

31
AML in CR1- three categories. Good-risk patients inv16, t(8;21), t(15;17) chemotherapy alone Relapse->achieving CR2 and cure with high-dose therapy (HDT). Standard-risk patients No unfavourable cytogenetics Remission after one course of chemotherapy matched sibling allograft-improve survival Poor-risk AML adverse cytogenetics: -5,-7,del(5q), abnormal 3q, failed remission induction and myelodysplasia have a low chance of cure with conventional therapy candidates for UD-SCT if they lack a sibling donor Role in AML
, t(15;17) chemotherapy alone Relapse->achieving CR2 and cure with high-dose therapy (HDT). Standard-risk patients No unfavourable cytogenetics Remission after one course of chemotherapy matched sibling allograft-improve survival Poor-risk AML adverse cytogenetics: -5,-7,del(5q), abnormal 3q, failed remission induction and myelodysplasia have a low chance of cure with conventional therapy candidates for UD-SCT if they lack a sibling donor Role in AML.")
33
Graft-versus-Host Disease (GVHD)
")
34
Stage Skin Liver Gut + Maculopapular rash Bilirubin Diarrhea <25% body surface 2-3 mg/dl 500-1,000ml/d persistent nausea* ++ Maculopapular rash Bilirubin Diarrhea 25-50% body surface 3-6 mg/dl 1,000-1,500ml/d +++ Generalized Bilirubin Diarrhea erythroderma 6-15 mg/dl >1,500ml/day ++++ Desquamation Bilirubin Pain or ileus and bullae > 15 mg/dl * Persistent nausea with histologic evidence of GVHD in the stomach or duodenum. Staging of Acute GVHD

35
HLA Disparity vs. Acute GVHD

36
Treatment of GVHD Stopping activation and proliferation of donor lymphocyte Steroids Cyclosporine Methotrexate Tacrolimus Sirolimus Mycophenolate mofetil Alemtuzamab (Campath) Anti-IL2 antibodies
 Anti-IL2 antibodies")


, PR(+) –HER-2: +3.>")


 14:00~17:30 ◇ 장 소 : 건강보험심사평가원 본원 지하대강당 ◇ 주 관 : 건강보험심사평가원.>")


 주요 내용 소개>")
 14: :00>")


![MGR review 류마티스 내과 R4 최인아. [ 목차 ] Overlap syndrome (vs UCTD, MCTD) Polymyositis(PM) PM with Interstitial lung disease.](/42/11353284/big_thumb.jpg "MGR review 류마티스 내과 R4 최인아. [ 목차 ] Overlap syndrome (vs UCTD, MCTD) Polymyositis(PM) PM with Interstitial lung disease.>")





- Agonists against Hepatitis B virus (HBV)-associated Hepatocellular.>")


