Download presentation
Presentation is loading. Please wait.

1
유방암 (Breast Cancer) 서울대학교병원 약제부 강래영 Rph, BCOP
 서울대학교병원 약제부 강래영 Rph, BCOP")
2
유방암 (Breast Cancer) 정의 : 여성의 유방내의 유선조직 ( 유관, 유엽 ) 의 상 피세포에서 발생하는 암 역학 : 발생율 국내 여성 2 위, 암사망원인 5 위, 2010 미국 여성 1 위, 암사망원인 2 위, 2010 선진국에서의 발생률이 높음 미국 여성, 평생 8 명 중 1 명에서 발생 서구여성의 경우 유방암이 60 대 이후의 상 대적 높은 연령대에서 호발 한국여성에서는 특징적으로 40 대의 비교적 젊은 나이에 많이 발생 남성에서도 발생 가능 5 년 생존률 : 89%, 국내 : 91% (06-10) 성별 10 대암 조발생률, 2010 년 여성 암사망률, 2011 Breast Cancer Risk Assessment Tool (www.cancer.gov/bcrisktool/Default.aspx)
 정의 : 여성의 유방내의 유선조직 ( 유관, 유엽 ) 의 상 피세포에서 발생하는 암 역학 : 발생율 국내 여성 2 위, 암사망원인 5 위, 2010 미국 여성 1 위, 암사망원인 2 위, 2010 선진국에서의 발생률이 높음 미국 여성, 평생 8 명 중 1 명에서 발생 서구여성의 경우 유방암이 60 대 이후의 상 대적 높은 연령대에서 호발 한국여성에서는 특징적으로 40 대의 비교적 젊은 나이에 많이 발생 남성에서도 발생 가능 5 년 생존률 : 89%, 국내 : 91% (06-10) 성별 10 대암 조발생률, 2010 년 여성 암사망률, 2011 Breast Cancer Risk Assessment Tool (")
3
유방암의 위험인자 (Risk Factor) 성별 ( 여성 -99%, 남성 -1%), 연령 내분비적 요인 –Total duration of menstrual life: 조기 초경 ( 55 세 ) –Nulliparity, a late age at first birth (30 세 이상 ) –Hormone replacement therapy ( 장기, Progesterone 병용 ) (Contraceptive? Risk/Benefit) 식이 요인 –Western diet (high calorie, fat, cooked meat) –High fat (steroid hormone metabolism 과의 상관성 ), saturated fat and meat intake, lower vegetable consumption –Phytoestrogens (controversial) 생활습관 요인 High BMI, 비만 음주, 방사선 노출 (40 세 이전 )
 식이 요인 –Western diet (high calorie, fat, cooked meat) –High fat (steroid hormone metabolism 과의 상관성 ), saturated fat and meat intake, lower vegetable consumption –Phytoestrogens (controversial) 생활습관 요인 High BMI, 비만 음주, 방사선 노출 (40 세 이전 ).")
4
유전적 요인 (5~10%) 개인력 : Contralateral breast cancer 의 가능성은 유방암 환자가 5 배 더 높음 가족력 (6-12%): 강력한 영향 요인 1 차 직계가족 : ~3 배 ( 연령에 따라 ) 직계가족이 45 세 이전에 유방암 발생한 경우 더 위험성 크다. 2 차 가족이 유방암이 있을 확률은 약 50% 증가 (RR=1.5) 모측과 부측의 가족력은 유사하게 영향을 미침 자궁과 난소암 환자의 경우 유방암 발생 위험성 증가 BRCA1 (long arm of chromsome 17, 17q21), BRCA2(chromosome 13) - Tumor suppressor gene – 의 비정상이 유방암 발생 위험 증가와 관련 있음 ( 확률 : 1/500) –BRCA1: 85% lifetime risk of breast cancer, 60% lifetime risk of ovary cancer (and colon cancer, prostate cancer ↑) –BRCA2: Similar breast cancer, lower ovarian cancer –Oophorectomy, Surgical Prophylaxis, Mammography Q 6 month 기타 증식성 섬유낭 변화는 유방암 위험도를 1.5~2 배 증가시키지만 비증식성 양성 유방질환, 섬유선종 등의 존재는 유방암의 위험성과 관련이 없다. Breast density: 위험성 증가 유방암의 위험인자 (Risk Factor)
 모측과 부측의 가족력은 유사하게 영향을 미침 자궁과 난소암 환자의 경우 유방암 발생 위험성 증가 BRCA1 (long arm of chromsome 17, 17q21), BRCA2(chromosome 13) - Tumor suppressor gene – 의 비정상이 유방암 발생 위험 증가와 관련 있음 ( 확률 : 1/500) –BRCA1: 85% lifetime risk of breast cancer, 60% lifetime risk of ovary cancer (and colon cancer, prostate cancer ↑) –BRCA2: Similar breast cancer, lower ovarian cancer –Oophorectomy, Surgical Prophylaxis, Mammography Q 6 month 기타 증식성 섬유낭 변화는 유방암 위험도를 1.5~2 배 증가시키지만 비증식성 양성 유방질환, 섬유선종 등의 존재는 유방암의 위험성과 관련이 없다. Breast density: 위험성 증가 유방암의 위험인자 (Risk Factor).")
5
병태생리 (Pathophysiology) Pathologic prognostic factor: Presence of necrosis, lymphatic or vascular invasion, nuclear grade, proliferative index, amount of aneuploidy, hormone receptor status, HER-2/neu gene amplification or protein expression Noninvasive Carcinoma (15~30%) –Preinvasive phase, carcinoma in situ –Malignant transformation of cells has occurred, but the basement membrane is intact –Ductal Carcinoma in Situ (DCIS) –Lobular Carcinoma in Situ (LCIS) Invasive Carcinoma
 Pathologic prognostic factor: Presence of necrosis, lymphatic or vascular invasion, nuclear grade, proliferative index, amount of aneuploidy, hormone receptor status, HER-2/neu gene amplification or protein expression Noninvasive Carcinoma (15~30%) –Preinvasive phase, carcinoma in situ –Malignant transformation of cells has occurred, but the basement membrane is intact –Ductal Carcinoma in Situ (DCIS) –Lobular Carcinoma in Situ (LCIS) Invasive Carcinoma")
6
Invasive or infiltrating ductal carcinoma (IDCa): 75% –Commonly spread to the axillary lymph nodes and their prognosis is poorer than for other histologic types (tubular, medullary, mucinous). Invasive or infiltrating lobular carcinoma (5-10%): ill-defined thickening in the breast, difficult to detect by mammography 두 군 사이에 axillary node involvement 나 재발, 사망 위험율은 유사 전이 부위에 차이가 있음 –Infiltrating ductal carcinoma (bone, liver, lung, brain,) –infiltrating lobular carcinoma (leptomeninges, peritoneal surfaces, retroperitoneum, gastrointestinal tract, reproductive organs) Medullary carcinoma (<7%) Mucinous carcinoma (3%) Tubular carcinoma (2%) Paget disease (1-4%): neoplastic cells in the nipple areolar complex. Phyllodes tumors Inflammatory breast cancer : mistaken for an infectious cellulitis or mastitis. 예후가 좋 지 않다. 병태생리 (Pathophysiology)
: ill-defined thickening in the breast, difficult to detect by mammography 두 군 사이에 axillary node involvement 나 재발, 사망 위험율은 유사 전이 부위에 차이가 있음 –Infiltrating ductal carcinoma (bone, liver, lung, brain,) –infiltrating lobular carcinoma (leptomeninges, peritoneal surfaces, retroperitoneum, gastrointestinal tract, reproductive organs) Medullary carcinoma (<7%) Mucinous carcinoma (3%) Tubular carcinoma (2%) Paget disease (1-4%): neoplastic cells in the nipple areolar complex. Phyllodes tumors Inflammatory breast cancer : mistaken for an infectious cellulitis or mastitis. 예후가 좋 지 않다. 병태생리 (Pathophysiology).")
7
스크리닝 유방 자가검진 : 매월 월경이 끝나고 3~5 일 후 ( 유방 이 가장 부드러움 ) - 먼저 거울에 비추어 자신의 유방 의 형태를 관찰하고, 한 손을 머리위로 올린 후 다른 한 손을 이용하여 가운데 세 손가락 끝 바닥을 이용 하여 유방을 촉진. 촉진은 유방을 부드럽게 누르면서 비비듯이 바깥쪽부터 원형을 그리면서 유두를 향하 여 실시. 멍울, 통증, 유두분비, 유두의 함몰, 유방의 주름, 유두습진, 유방 피부 변화와 같은 사항을 주의 깊게 보아야 함 국내 여성 유방암 환자의 약 1/3 은 정기 검진 중에 발견된 다.

8
유방암의 임상 증상 무증상 유방종괴 (A painless, palpable lump) – 70% 즉 유방에 멍울이나 혹이 만져지는 증상 유방암이 아닌 섬유선종이나 섬유낭종과 같은 양성질환과 감별 유방통 유방에 생기는 통증이나 불편감, 여성 호르몬에 의한 정상적인 생 리현상인 경우가 많고 유방암의 유일한 증상인 경우는 드물다. 유두분비 (nipple discharge) 유두함몰 (nipple retraction, dippling), 유두의 습진성 변화 유방의 피부변화 (skin edema, redness, warmth): 피부함몰, 피부궤 양, 피부 결절 겨드랑이 림프절 촉지 (Palpable local–regional lymph nodes)
 유두함몰 (nipple retraction, dippling), 유두의 습진성 변화 유방의 피부변화 (skin edema, redness, warmth): 피부함몰, 피부궤 양, 피부 결절 겨드랑이 림프절 촉지 (Palpable local–regional lymph nodes).")
9
진단 및 검사 영상검사 – 유방촬영술 (Mammography): 가장 기본이 되는 검사, 일반적으로 상하, 좌우의 2 가지 종류의 x-ray 사진, 유방 내의 유선조직이 풍부한 치밀유방 의 경우 검사의 정확도 감소 – 유방초음파 : 유선조직이 풍부한 치밀유방에서 유방촬영술에서 보이지 않 는 종괴를 발견하는 데 유용 – 자기공명영상 (MRI) 조직검사 – 미세침 흡인 생검 (Fine needle aspiration) – 중앙부 절침생검 (Core-needle biopsy) – 절제생검 (Excisional biopsy) – 맘모톰 조직검사 (Mammotome Biopsy)
: 가장 기본이 되는 검사, 일반적으로 상하, 좌우의 2 가지 종류의 x-ray 사진, 유방 내의 유선조직이 풍부한 치밀유방 의 경우 검사의 정확도 감소 – 유방초음파 : 유선조직이 풍부한 치밀유방에서 유방촬영술에서 보이지 않 는 종괴를 발견하는 데 유용 – 자기공명영상 (MRI) 조직검사 – 미세침 흡인 생검 (Fine needle aspiration) – 중앙부 절침생검 (Core-needle biopsy) – 절제생검 (Excisional biopsy) – 맘모톰 조직검사 (Mammotome Biopsy)")
10
Staging ( 병기 ) American Joint Committee on Cancer (AJCC) TMN Staging
 American Joint Committee on Cancer (AJCC) TMN Staging")
11
Staging ( 병기 ) sentinel lymph node ( 감 시 림프절 ): 유방내의 암 으로부터 림프액이 처음 으로 배액되어 암세포의 전이가 가장 먼저 이루 어지는 림프절
 sentinel lymph node ( 감 시 림프절 ): 유방내의 암 으로부터 림프액이 처음 으로 배액되어 암세포의 전이가 가장 먼저 이루 어지는 림프절")
12
Staging: AJCC

13
Prognosis [ 유방암의 병기별 5 년 생존율 ] [ 중앙암등록본부 2008 년통계 ] 병기 0기0기 1기1기 2기2기 3기3기 4기4기 5 년 생존율 100%98.4%91.6%69.7%30.2% 내용 상피내암 ( 암세포가 유 선 내에 국한 되어 있는 경 우 ) 종괴 크기가 2cm 미만이고 림프절 전이 가 없는 경우 0,1,3,4 기에 해당되지 않 는 나머지 종괴 크기가 5cm 이상이고 전이가 약간 있는 경우나 림프절 전이가 심 한 경우 뼈, 폐, 간 등 의 전신 전이 가 동반된 경 우 재발률 : 약 25~30% a Confined to primary site. Includes stages I and II. b Regional spread to lymph nodes or directly beyond primary site. Includes stages II and III. c Distant metastasis. Stage IV. d With conventional local and systemic therapy. Based on November 2008 SEER data TABLE 136-5
![Prognosis [ 유방암의 병기별 5 년 생존율 ] [ 중앙암등록본부 2008 년통계 ] 병기 0기0기 1기1기 2기2기 3기3기 4기4기 5 년 생존율 100%98.4%91.6%69.7%30.2% 내용 상피내암 ( 암세포가 유 선 내에 국한 되어 있는 경 우 ) 종괴 크기가 2cm 미만이고 림프절 전이 가 없는 경우 0,1,3,4 기에 해당되지 않 는 나머지 종괴 크기가 5cm 이상이고 전이가 약간 있는 경우나 림프절 전이가 심 한 경우 뼈, 폐, 간 등 의 전신 전이 가 동반된 경 우 재발률 : 약 25~30% a Confined to primary site.](http://images.slidesplayer.org/47/11665191/slides/slide_13.jpg "Includes stages I and II. b Regional spread to lymph nodes or directly beyond primary site. Includes stages II and III. c Distant metastasis. Stage IV. d With conventional local and systemic therapy. Based on November 2008 SEER data TABLE")
14
Poor prognosis 와 관련된 인자 Age < 35 years Alcohol (> 6 g/day) High fat diet (esp, estrogen receptor (-) breast cx), no exercise Tumor size, lymph node status Histologic type (Ductal, Lobular > Mucinous, Tubular) Inflammatory breast cancer (Clinical) High nuclear grade and histologic differentiation.. Tumor is growing quickly: Grade 1 (well differentiated), Grade 2 (moderately differentiated), Grade 3 (poorly differentiated) Lymphatic and vascular invasion Negative Tumor receptor Status (ER (-), PR (-), HER2-) Overexpression of HER-2/neu (20-30%) –HER status measuring: FISH (positive, equivocal, negative), IHC (0, 1+, 2+, 3+) –Trastuzumab 치료에 따라서 outcome 달라짐 High Proliferation marker: Ki-67 Oncotype DX assay, MammaPrint
, Grade 2 (moderately differentiated), Grade 3 (poorly differentiated) Lymphatic and vascular invasion Negative Tumor receptor Status (ER (-), PR (-), HER2-) Overexpression of HER-2/neu (20-30%) –HER status measuring: FISH (positive, equivocal, negative), IHC (0, 1+, 2+, 3+) –Trastuzumab 치료에 따라서 outcome 달라짐 High Proliferation marker: Ki-67 Oncotype DX assay, MammaPrint.")
15
치료 (Treatment) In situ tumor or Stages I, II : Cure - Surgery Alone (In situ-most, Stage I-70~80%, Stage II -50%) Locally advanced breast cancer, Stage III: Cure - Combination of Surgery, Radiation, and Chemotherapy (Neoadjuvant, Adjuvant) Metastatic breast cancer: improve symptom, maintain QOL, prolong survival - Cytotoxic chemotherpay, Endocrine therapy Desired Outcome
 In situ tumor or Stages I, II : Cure - Surgery Alone (In situ-most, Stage I-70~80%, Stage II -50%) Locally advanced breast cancer, Stage III: Cure - Combination of Surgery, Radiation, and Chemotherapy (Neoadjuvant, Adjuvant) Metastatic breast cancer: improve symptom, maintain QOL, prolong survival - Cytotoxic chemotherpay, Endocrine therapy Desired Outcome")
16
Early Breast Cancer (Stage I, II) Local–Regional Therapy Radical mastectomy –Removal of the breast and both major and minor pectoralis muscles –Ipsilateral axillary nodes removal, external beam radiation therapy –Substantial morbidity: decreases strength and range of motion, edema of the arm and resected breast area Modified radical mastectomy = total mastectomy with axillary lymph node dissection –Standard surgical approach in the 1970s –Pectoralis minor muscle may be excised, divided, or left intact –Variation in the extent of axillary lymph node dissection, ranging from sampling to full dissection – 종양이 5cm 이상이거나 절제 가장자리가 양성 또는 1mm 미만으로 근접해있는 경우, 흉벽 에 대한 방사선 요법으로 시행해야 한다. Breast-conserving therapy –removal of part of the breast, surgical evaluation of the axillary lymph node basin, and radiation therapy to the breast ; appropriate, primary method of primary therapy for stage I and stage II breast cancer –Wide local excision –Lumpectomy –Quadrantectomy – 모든 환자에서 전체 유방에 방사선 요법을 시행해야 한다.

17
Early Breast Cancer (Stage I, II) Systemic Adjuvant Therapy Administration of systemic therapy following definitive local therapy (surgery, radiation, or a combination of these) when there is no evidence of metastatic disease, but a high likelihood of disease recurrence d/t micrometastasis Goal of systemic adjuvant therapy: cure Recommend –All patients with positive hormone receptor status, regardless of age, menopausal status, involvement of axillary lymph nodes, or tumor size. ( 예외, 림프절 음성이면서 0.5cm 이하의 종양 ) –All patients with lymph node metastases or with primary breast cancers larger than 1 cm in diameter (both node-negative and node-positive)
 –All patients with lymph node metastases or with primary breast cancers larger than 1 cm in diameter (both node-negative and node-positive).")
18
General Approach to Treatment Decision to adjuvant therapy Oncotype DX (low recurrence score (<18), high recurrence score (≥ 31) MammaPrint Adjuvant! (www.adjuvantonline.com) Tumors <1 cm, micrometastatic lymph node involvement, or negative lymph nodes treatment is highly individualized and based on multiple patient- and tumor-related factors, including HR status, HER2 status, concomitant comorbidities, patient preference.

19
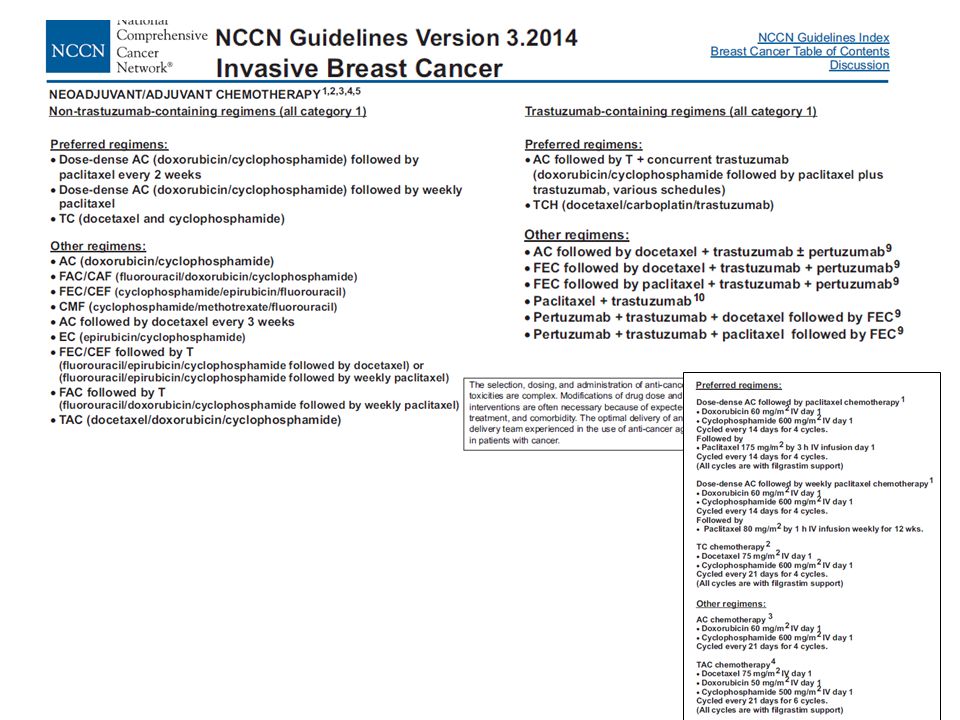
(Neo) Adjuvant Chemotherapy 2-3 가지의 약제를 복합하여 사용하는 것이 효과적, 총 4-8 주기의 치료를 시행하게 됨 ( 일반적으로 12-24 주 ) Cytotoxic chemotherapy is a particularly important treatment modality for patients with tumors that do not express ER or PR and do not overexpress HER2 (so called triple-negative breast cancers, TNBC)
 Adjuvant Chemotherapy 2-3 가지의 약제를 복합하여 사용하는 것이 효과적, 총 4-8 주기의 치료를 시행하게 됨 ( 일반적으로 주 ) Cytotoxic chemotherapy is a particularly important treatment modality for patients with tumors that do not express ER or PR and do not overexpress HER2 (so called triple-negative breast cancers, TNBC)")
20
Adjuvant Biological Therapy –Trastuzumab: monoclonal antibody targeted against the HER2- receptor protein –HER-2/neu overexpression: Resistant to alkylating agent, greater benefit from an anthracycline based therapy –HER-2/neu receptor overexpression: poor prognosis –50% reduction in the risk of recurrence –Node(+) 또는 T >1cm 인 HER-2(+) 환자에서 권고 (Neo) Adjuvant Biological Therapy
 또는 T >1cm 인 HER-2(+) 환자에서 권고 (Neo) Adjuvant Biological Therapy")
22
목표 : (a) decrease circulating levels of estrogen (b) prevent the effects of estrogen at the breast cancer cell (targeted therapy) by blocking the hormone receptors or downregulating the presence of those receptors Hormone Receptor status: indicators of prognosis and predictor of response to endocrine therapy HR (+): ER (+) /PR (+); longer disease free interval between primary and metastasis, favorable prognosis, superior response to hormone therapy, postmenopausal>premenopausal No combination endocrine therapy Sequential use of endocrine agents Duration of treatment: 5 years, beyond 5 years Anti-estrogen: Tamoxifen, Toremifen; Premenopausal, Postmenopausal Aromatase Inhibitors: Anastrozole, Letrozole : Postmenopausal Dosing Method –Upfront adjuvant hormonal therapy (AI or Tamoxifen for 5 years) –AI 5years after 5 years of adjuvant tamoxifen therapy (Extended) –Sequential use after 2 to 3 years of adjuvant tamoxifen, total 5 years Adjuvant Endocrine Therapy
 decrease circulating levels of estrogen (b) prevent the effects of estrogen at the breast cancer cell (targeted therapy) by blocking the hormone receptors or downregulating the presence of those receptors Hormone Receptor status: indicators of prognosis and predictor of response to endocrine therapy HR (+): ER (+) /PR (+); longer disease free interval between primary and metastasis, favorable prognosis, superior response to hormone therapy, postmenopausal>premenopausal No combination endocrine therapy Sequential use of endocrine agents Duration of treatment: 5 years, beyond 5 years Anti-estrogen: Tamoxifen, Toremifen; Premenopausal, Postmenopausal Aromatase Inhibitors: Anastrozole, Letrozole : Postmenopausal Dosing Method –Upfront adjuvant hormonal therapy (AI or Tamoxifen for 5 years) –AI 5years after 5 years of adjuvant tamoxifen therapy (Extended) –Sequential use after 2 to 3 years of adjuvant tamoxifen, total 5 years Adjuvant Endocrine Therapy")
23
Locally Advanced Breast Cancer (Stage III) Diagnosed in patients who have had symptoms for months to years and have neglected to seek medical attention. Poor prognosis because of the delay in diagnosis Neoadjuvant chemotherapy: 근치적 수술이 어려운 환자 (N2-3 or T4) 에서 반응을 유도하여 수술이나 방사선치료 등 국소치료가 가능하도 록 한다, 근치적 수술이 가능한 환자 (T3N1M0) 에서는 유방보존수술 이 가능하게 한다. *Same regimen with adjuvant setting Primary chemotherapy with an anthracycline-containing regimen with or without a taxane HER2-positive tumors: trastuzumab with chemotherapy Neoadjuvant endocrine therapy: patients who have unresectable hormone receptor-positive tumors who are unable to receive chemotherapy (4~6 개월 ) Adjuvant radiation therapy: all locally advanced breast cancer patients to minimize local recurrences.
 에서 반응을 유도하여 수술이나 방사선치료 등 국소치료가 가능하도 록 한다, 근치적 수술이 가능한 환자 (T3N1M0) 에서는 유방보존수술 이 가능하게 한다. *Same regimen with adjuvant setting Primary chemotherapy with an anthracycline-containing regimen with or without a taxane HER2-positive tumors: trastuzumab with chemotherapy Neoadjuvant endocrine therapy: patients who have unresectable hormone receptor-positive tumors who are unable to receive chemotherapy (4~6 개월 ) Adjuvant radiation therapy: all locally advanced breast cancer patients to minimize local recurrences..")
24
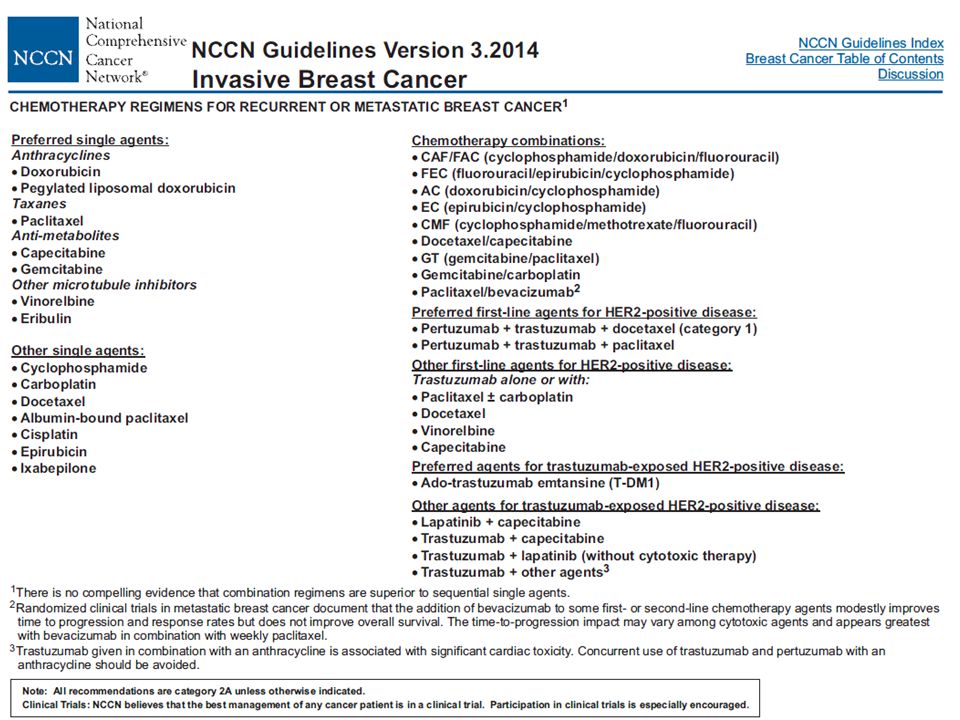
Metastatic Breast Cancer (Stage IV) The choice of therapy for metastatic disease is based on the site of disease involvement and HR status in the primary tumor tissue. HR (+): Endocrine therapy → (if fail) Chemotherapy Endocrine therapy: treatment of choice for patients with HR(+) with metastatic disease in soft tissue, bone, or pleura –median duration of response: 9-12 month –Tamoxifen –Newer generation of AI: less toxic than first generation, superior to tamoxifen as first- line therapy for advanced breast cancer in postmenopausal women Cytotoxic Chemotherapy : HR (-) with rapidly progressing, metastasis to liver, lung, CNS, progressed on initial endocrine therapy –Symptomatic visceral and/or central nervous system involvement generally have more rapidly growing cancers that require chemotherapy. –CR (20%), PR (most), median duration of response: 5-12 month HER2 protein overexpression (+): HER2-targeted therapy alone or with chemotherapy or endocrine therapy All breast cancer patients with metastases to the bone should be considered for treatment with an intravenous bisphosphonate (e.g., pamidronate or zoledronic acid)
: Endocrine therapy → (if fail) Chemotherapy Endocrine therapy: treatment of choice for patients with HR(+) with metastatic disease in soft tissue, bone, or pleura –median duration of response: 9-12 month –Tamoxifen –Newer generation of AI: less toxic than first generation, superior to tamoxifen as first- line therapy for advanced breast cancer in postmenopausal women Cytotoxic Chemotherapy : HR (-) with rapidly progressing, metastasis to liver, lung, CNS, progressed on initial endocrine therapy –Symptomatic visceral and/or central nervous system involvement generally have more rapidly growing cancers that require chemotherapy. –CR (20%), PR (most), median duration of response: 5-12 month HER2 protein overexpression (+): HER2-targeted therapy alone or with chemotherapy or endocrine therapy All breast cancer patients with metastases to the bone should be considered for treatment with an intravenous bisphosphonate (e.g., pamidronate or zoledronic acid).")
25
재발 및 전이 유방암 진료 흐름도

27
SPECIFIC AGENTS USED IN BREAST CANCER

28
MOA: antiestrogen, selective estrogen receptor modulators (SERM) Both pre- and postmenopausal women Dose & Duration: 20 mg/day, 5 years Timing: after surgery or after completion of chemotherapy (sequential with chemotherapy; DFS advantage) PK/PD: –Prodrug, metabolized through multiple enzymes including CYP3A4, CYP2C19, CYP2D6 to active metabolites (endoxifen, more active than the parent compound) –Formation of endoxifen is highly dependent on the enzymatic activity of CYP2D6, Polymorphisms in CYP2D6 –Half life: 7 days (during chronic dosing) –Serum level detected 6 weeks after discontinuation of therapy –Max beneficial effects; at least 2 months following initiation Tamoxifen
 Both pre- and postmenopausal women Dose & Duration: 20 mg/day, 5 years Timing: after surgery or after completion of chemotherapy (sequential with chemotherapy; DFS advantage) PK/PD: –Prodrug, metabolized through multiple enzymes including CYP3A4, CYP2C19, CYP2D6 to active metabolites (endoxifen, more active than the parent compound) –Formation of endoxifen is highly dependent on the enzymatic activity of CYP2D6, Polymorphisms in CYP2D6 –Half life: 7 days (during chronic dosing) –Serum level detected 6 weeks after discontinuation of therapy –Max beneficial effects; at least 2 months following initiation Tamoxifen")
29
Potent inhibitor of CYP2D6 (paroxetine, fluoxetine, …), decrease levels of endoxifen → Avoid known strong inhibitors of CYP2D6 S/E: Endometrial Ca (RR 2.53), thromboembolism, stroke, hot flashes, vaginal discharge, Tumor flare and/or hypercalcemia (metastatic disease) Reduce fracture Monitoring: Regular gynecologic examinations Tamoxifen SERM, Lower estrogenic-to anti-estrogenic ratio as compared to tamoxifen Dose: 60 mg QD Indication: alternative to tamoxifen in patients with metastatic breast cancer Toremifene
, decrease levels of endoxifen → Avoid known strong inhibitors of CYP2D6 S/E: Endometrial Ca (RR 2.53), thromboembolism, stroke, hot flashes, vaginal discharge, Tumor flare and/or hypercalcemia (metastatic disease) Reduce fracture Monitoring: Regular gynecologic examinations Tamoxifen SERM, Lower estrogenic-to anti-estrogenic ratio as compared to tamoxifen Dose: 60 mg QD Indication: alternative to tamoxifen in patients with metastatic breast cancer Toremifene")
30
MOA: Inhibition of Aromatase that catalyze the conversion of androstenedione into estrone and estradiol, reduce the levels of circulating estrogens and estrogens in the target organ. Newer generation: Anastrozole, Letrozole, Exemestane : Similar effect Postmenopausal women Only Choice for Postmenopausal hormone-sensitive breast cancers A/E –bone loss/osteoporosis (Bisphosphonates co-administration) –hot flashes, vaginal dryness/atrophy –myalgia/arthralgia –mild headaches, diarrhea –hypercholesterolemia Aromatase Inhibitors (AIs)
 –hot flashes, vaginal dryness/atrophy –myalgia/arthralgia –mild headaches, diarrhea –hypercholesterolemia Aromatase Inhibitors (AIs).")
31
Other Endocrine Therapy LHRH-agonists Premenstraual Patients Means of Ovarian Ablation alternative to oophorectomy Goserelin (Zoladex®), Leuprorelin (Leuplin®) Hot flashes, amenorrhea menopausal symptoms, injection site reactions (extended formulations of more than 28 days are not recommended for the treatment of breast cancer) SERD: Fulvestrants Pure antiestrogen, bind to the ER, inhibit estrogen binding, and degrade the drug-ER complex second-line therapy of postmenopausal metastatic breast cancer patients 500 mg, IM injection every 28 days injection-site reactions, hot flashes, asthenia, and headaches
, Leuprorelin (Leuplin®) Hot flashes, amenorrhea menopausal symptoms, injection site reactions (extended formulations of more than 28 days are not recommended for the treatment of breast cancer) SERD: Fulvestrants Pure antiestrogen, bind to the ER, inhibit estrogen binding, and degrade the drug-ER complex second-line therapy of postmenopausal metastatic breast cancer patients 500 mg, IM injection every 28 days injection-site reactions, hot flashes, asthenia, and headaches")
32
Progestins megestrol acetate, medroxyprogesterone acetate Third-line therapy after patients have failed an AI and an antiestrogen (tamoxifen, toremifene, or fulvestrant). Megestrol acetate 160 mg/day S/E: weight gain, fluid retention, vaginal bleeding, hot flashes, thromboembolism Other Endocrine Therapy

33
Anthracyclines: Doxorubicin= Adriamycin Topoisomerase II inhibitor Doxorubicin, Idarubicin, Epirubicin, Daunorubicin, ….. Cardiac Toxicity –< 1%, total cumulative doxorubicin dose < 320 mg/m 2 – 최대 축적 총투여량 : Doxorubicin 550 mg/m 2 – 종격 부위에 방사선 치료를 행한 경우 최대 축적 총투여량 : 450 mg/m 2 – 약물투여전 심초음파 검사를 시행하여 좌심실의 심박출량이 (LVEF: Left Ventricle Ejection Fraction) 30-40% 인 경우에는 약물 투여를 시행해서는 안된 다. Myelosuppression (DLT) High Emetic Potential Extravasation Alopecia 뇨색 변색 간장애, 골수억제시 용량조절 구토 발현율 20 mg 이하 : 10-30 % 20-75 mg : 30-60 % 75 mg 이상 : 60-90 %
 30-40% 인 경우에는 약물 투여를 시행해서는 안된 다. Myelosuppression (DLT) High Emetic Potential Extravasation Alopecia 뇨색 변색 간장애, 골수억제시 용량조절 구토 발현율 20 mg 이하 : % mg : % 75 mg 이상 : %.")
34
Cyclophosphamide Alkylating agent 간의 cytochrome P450 에 의해 가수분해되어 중간 대사체인 4- hydroxycyclophosphamide 와 aldophosphamide 로 대사된 후, 항종양 활성을 지닌 알킬화제인 acrolein 과 phosphoramide mustard 로 산화됨, 이 활성형 대 사체가 DNA 사슬을 알킬화시키고 교차결합을 통해 종양조직 및 정상 조직의 성장을 저해함 출혈성 방광염 (7-40%): 환자의 7-12% ( 연구에 따라서는 약 40% 까지 ) 에서 발생. 대개 심각하며 치명적일 수도 있으며, 대사체인 acrolein 이 방광을 화학 적으로 자극하여 나타난다고 여겨짐. 치료 기간 중에는 다량의 물 ( 매일 3-4 L) 을 섭취하도록 하고 자주 소변을 보게 하며, 본 약물을 야간에 투여하지 않도 록 한다. 고용량, 주사의 경우 mesna 투여 가능 골수 억제 오심, 구토 ( 고용량 ) 탈모 불임, 무월경증 황달
 을 섭취하도록 하고 자주 소변을 보게 하며, 본 약물을 야간에 투여하지 않도 록 한다. 고용량, 주사의 경우 mesna 투여 가능 골수 억제 오심, 구토 ( 고용량 ) 탈모 불임, 무월경증 황달.")
35
Taxane: Paclitaxel (Taxol®), Docetaxel (Taxotere®) Antimicrotubule agent Myelosuppression (DLT); 골수억제 ( 용량의존적, 주입 속도 의존적 : 고용량에서, 더 빈번한 횟수에서, infusion 기간이 길수록 증가 ) – 발현 (Onset): 8-10 일 – 최저치 (Nadir): 11 일 – 회복 (Recovery): 15-21 일 Hypersensitivity reaction (Premedication: diphenhydramine, famotidine, hydrocortisone) Peripheral neuropathy Myalgias, arthralgias (NSAIDS) Alopecia ( 완전탈모 ) Low emetogenic potential Fluid Retention (Docetaxel): dexamethasone 전처치 : 수분 저류의 빈 도, 중증도 감소. 과민반응 감소 Docetaxel: 조제 후 6 시간 안정 Weekly / Three weekly Regimen

36
Eribulin (Halaven®) non-taxane microtubule inhibitor 합성 halichondrin B 유도체로 microtubule 억제 적응증 : anthracycline 계, taxane 계 약물을 포함하는 최소 두 가지의 화학요법 치료를 받은 적이 있는 국소 진행성 혹은 전이성 유방암 환 자의 단일 치료 요법 용량, 용법 : 1.4mg/m 2 IV bolus 2~5 min D1, D8 q3wk 부작용 Myelosuppression peripheral neuropathy fatigue, athralgia/myalgia, back pain, alopecia,
 non-taxane microtubule inhibitor 합성 halichondrin B 유도체로 microtubule 억제 적응증 : anthracycline 계, taxane 계 약물을 포함하는 최소 두 가지의 화학요법 치료를 받은 적이 있는 국소 진행성 혹은 전이성 유방암 환 자의 단일 치료 요법 용량, 용법 : 1.4mg/m 2 IV bolus 2~5 min D1, D8 q3wk 부작용 Myelosuppression peripheral neuropathy fatigue, athralgia/myalgia, back pain, alopecia,")
37
Monoclonal antibody targeted against the HER2-receptor protein 1 주 요법 – 초기부하용량 : 4mg/kg, 90 분간 투여 – 유지용량 : 매주 2mg/kg 씩, 초기부하용량 투여 1 주 후부터 투여를 시작한다. 3 주 요법 – 초기부하용량 : 8mg/kg – 유지용량 : 6mg/kg 을 초기부하용량 투여 3 주 후부터 투여 시작한다. (Adjuvant therapy) 1 년간 치료 유지 Cardiotoxicity: Anthracycline 과 병용시 심함 ; 약물 투여 전, 투여 중 에 left ventricular function 평가필요하며 LVEF 심한 감소가 나타나는 경우 약물 투여 중단 Infusion Reaction ( 첫 회 투여시 40% 특히 ): 발열, 오한, 오심, 구토, 통증, 떨림, 두통, 어지러움, 발진, 무기력, 경증, 중등도의 경우 중단하지 않고 acetaminophen 으로 치료 가능, 투여속도 조절 필요 Trastuzumab (Herceptin®)
 1 년간 치료 유지 Cardiotoxicity: Anthracycline 과 병용시 심함 ; 약물 투여 전, 투여 중 에 left ventricular function 평가필요하며 LVEF 심한 감소가 나타나는 경우 약물 투여 중단 Infusion Reaction ( 첫 회 투여시 40% 특히 ): 발열, 오한, 오심, 구토, 통증, 떨림, 두통, 어지러움, 발진, 무기력, 경증, 중등도의 경우 중단하지 않고 acetaminophen 으로 치료 가능, 투여속도 조절 필요 Trastuzumab (Herceptin®).")
38
Pertuzumab (Perjeta ®) Humanized monoclonal antibody to HER-2 Pertuzumab : HER2 의 sub-domain2 에 결합하여 HER2 와 HER3 또 는 EGFR 등의 heterodimerization 을 저해 cf) Trastuzumab: HER2 의 sub-domain4 에 결합하여 HER2-HER2 homodimerization 을 저해 HER2+ 환자의 1 차 치료 Pertuzumab + trastuzumab + docetaxel (category 1) Pertuzumab + trastuzumab + Paclitaxel 용량 : LD 840mg ov60mins, MD 420mg ov30-60mins q3wk ( 투약간격 6 주 이상시, 다시 초회용량 840mg 을 투여 )
 Humanized monoclonal antibody to HER-2 Pertuzumab : HER2 의 sub-domain2 에 결합하여 HER2 와 HER3 또 는 EGFR 등의 heterodimerization 을 저해 cf) Trastuzumab: HER2 의 sub-domain4 에 결합하여 HER2-HER2 homodimerization 을 저해 HER2+ 환자의 1 차 치료 Pertuzumab + trastuzumab + docetaxel (category 1) Pertuzumab + trastuzumab + Paclitaxel 용량 : LD 840mg ov60mins, MD 420mg ov30-60mins q3wk ( 투약간격 6 주 이상시, 다시 초회용량 840mg 을 투여 )")
39
참고 Pharmacotherapy: A Pathophysiologic Approach, 8th Edition 국가암정보센터 (www.cancer.go.kr)www.cancer.go.kr 식약처 온라인 의약도서관 (http://drug.mfds.go.kr)http://drug.mfds.go.kr 식약처 의약품 전자민원창구 (http://ezdrug.mfds.go.kr) 건강보험심사평가원 (www.hira.or.kr)www.hira.or.kr 정보 > 약제정보 > 약제급여기준정보 > 암질환사용약제 > 항암화학요법 The National Comprehensive Cancer Network (NCCN) (www.nccn.org)www.nccn.org Uptodate® (www.uptodate.com)
 ( Uptodate® (")
Similar presentations


, PR(+) –HER-2: +3.>")
 HER2/neu, EGFR, k-ras, c-kit II.High-throughput.>")



 주요 내용 소개>")
 –Leptin: apheliotrophic actions Atherosclerosis,>")





>")


>")

