Download presentation
Presentation is loading. Please wait.

1
Shock의 원인 Cardiogenic shock: hypovolemic shock Septic shock
pericardial tamponade, constrictive heart failure, massive hydrothorax, positive pressure ventilation, diaphragmatic hernia hypovolemic shock Massive bleeding ( GI , liver , spleen ... ) , Septic shock pneumonia, enteritis 등의 모든 감염성 질환 Neurogenic shock spinal anesthesia, severe head injury, spinal cord injury, pharmacotherapy
 , Septic shock. pneumonia, enteritis 등의 모든 감염성 질환. Neurogenic shock. spinal anesthesia, severe head injury, spinal cord injury, pharmacotherapy.")
3
Hypovolemic shock Shock은 항상 ATLS class에 따라서 진행되지 않는다
Not until patients are in class III shock does BP supposedly decrease. A common mistake is to think that trauma patients are often hypotensive; hypotension is rare in trauma patients. uncontrolled bleeding을 발견하는 것이 중요하고, 무엇보다도 class III shock에 빠지기 전에 bleeding을 멈추게 하는 것이 중요하다.(즉, 저혈압이 나타나기 전에 먼저 의심하여 치료하자.) blood loss를 replace하는 것보다 blood loss를 발견하는 것이 더 중요하다. 출혈이 있을 때, relative bradycardia가 있으면 mortality가 낮아진다. Relative bradycardia: SBP<90mmHg일 때 HR<100/min인 경우 HR 60-90일 때만 survival rate가 증가한다 (patients with a heart rate lower than 60 beats/min are usually moribund)
 blood loss를 replace하는 것보다 blood loss를 발견하는 것이 더 중요하다. 출혈이 있을 때, relative bradycardia가 있으면 mortality가 낮아진다. Relative bradycardia: SBP<90mmHg일 때 HR<100/min인 경우. HR 60-90일 때만 survival rate가 증가한다 (patients with a heart rate lower than 60 beats/min are usually moribund)")
4
Hypovolemic shock Arterial bleeding
Often stops temporarily on its own d/t spasm &thrombose Lacerated artery can bleed more than as transected artery ∵ Spasm에 의해 혈관의 구멍이 더 커짐 Results in rapid hypotension :because the arterial system is valveless, the recorded BP drops early, even before large-volume loss occurs. Venous bleeding : sometimes large volumes of blood are lost before hypotension ensues Slower, human body compensates Time for lactate, base deficit become abnormal Hct, Hb level 높거나 정상 Hb인 경우에도, significant bleeding이 있는 경우 있다 Hb수치가 낮은 경우, 대개 실제 Hb level과 blood loss의 정도를 반영한다. 또한, acellular fluid 투여하면 dilution이 생겨 Hb 수치가 더 떨어진다. 임상적으로 응급상황에서 full drop fluid 1L 당 1씩 감소

5
Septic shock

6
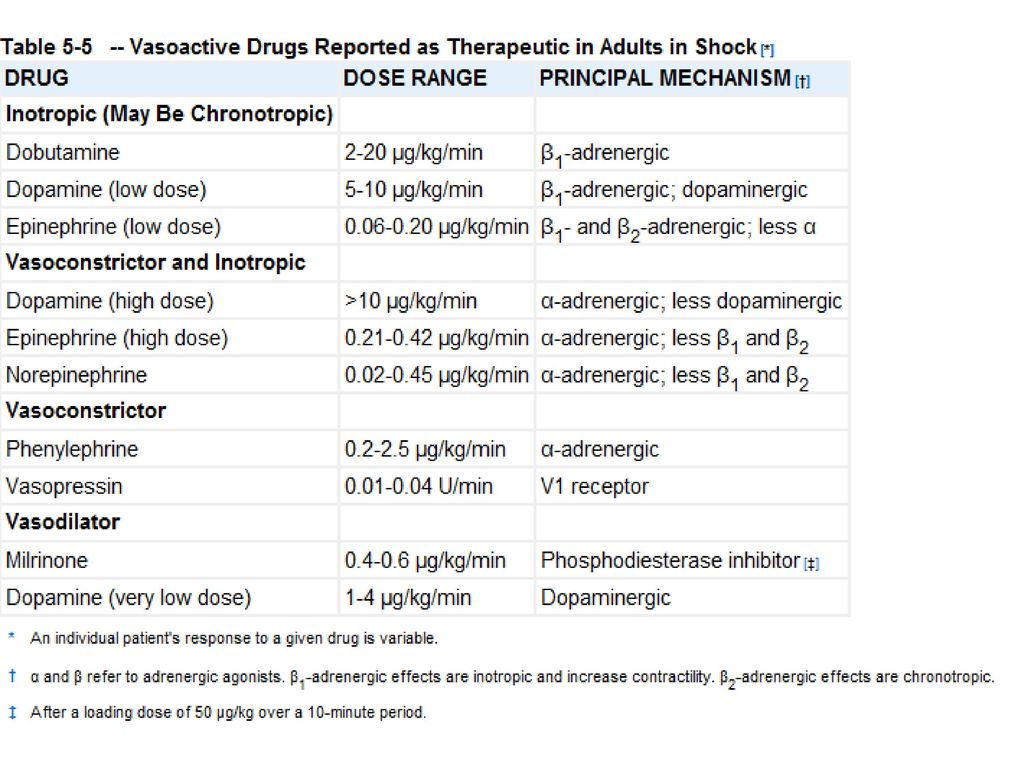
Cardiogenic shock

7
Cardiogenic shock Shock from AMI
7-10%(AMI)는 cardiogenic shock, 그중 70%는사망 initial angina 증상후 6-12시간후shock 증상시작 acute occlusion ⇒ LV wall poor contractility ⇒ ventricular chamber pressure↓⇒cardiacEF↓ 그외 acute MR, rupture of interventricular septum, rarely right ventricle dysfunction Systolic BP<90mmHg, distended neck vein, dyspnea with rale Gray on cyanotic face, diaphoresis, vasoconstricted extremities,and weakly palpable pulse decreased level of consciousness PCWP > 20mmHg, CI < 2.0l/mm/m2 치료; oxygen, NTG, aspirin, adequate IV morphine, Intraaortic balloon pump fibrinolytic therapy(tPA) antiplatelet treatment(glycoprotein IIb/IIIa) ⇒ improve patency of coronary stent graft immediate revascularization by endovascular treatment or CABG
는 cardiogenic shock, 그중 70%는사망. initial angina 증상후 6-12시간후shock 증상시작. acute occlusion ⇒ LV wall poor contractility ⇒ ventricular chamber pressure↓⇒cardiacEF↓ 그외 acute MR, rupture of interventricular septum, rarely right ventricle dysfunction. Systolic BP<90mmHg, distended neck vein, dyspnea with rale. Gray on cyanotic face, diaphoresis, vasoconstricted extremities,and weakly palpable pulse. decreased level of consciousness. PCWP > 20mmHg, CI < 2.0l/mm/m2. 치료; oxygen, NTG, aspirin, adequate IV morphine, Intraaortic balloon pump. fibrinolytic therapy(tPA) antiplatelet treatment(glycoprotein IIb/IIIa) ⇒ improve patency of coronary stent graft. immediate revascularization by endovascular treatment or CABG.")
8
Hyponatremia Mild 130-138, moderate 120-130 no signs or symptoms
Severe <120 mEq/L osmolality falling, cells are swelling Intracranial cell swelling: headaches, lethargy, coma or seizures 원인 Renal: renal failure, problems with ADH, diuretics Extrarenal: sodium loss caused by wounds, burns, sweating, congestive heart failure, cirrhosis, hypothyroidism, GI losses, cerebral salt wasting syndrome

9
Hyponatremia Treatments
Hypovolemic hyponatremia - Infuse isotonic saline to expand a contracted ECF volume, 등장성 수액으로 용적 부족을 우선 교정하고 진행 중인 소실을 보충. SIADH – 먼저 하루 1L 이내로 수분 제한. 반응 없다면, furosemide, mannitol 등의 투여가 필요. Hypervolemichyponatremia– 수분제한. 또는 furosemide 주입+3% NaCl로 요나트륨소실을 보충. 증상이 있거나 심각한 저나트륨혈증(<110)이 있을 때, 3%NaCl 고장성 수액이 필요.
이 있을 때, 3%NaCl 고장성 수액이 필요.")
10
Hypernatremia Most common cause : water loss
Ex : 더운 환경에서 땀을 많이 흘리고 수분 보충을 하지 않았을 때, or GI fluid loss Neurologic damage : altered level of consciousness, seizures, coma and intracerebral hemorrhage ECF volume 감소의 임상 지표: postural hypotension, dry mucus membranes, decresed skin turgor

11
Hypokalemia [K+] < 3.5mmol/L hyperpolarization of the resting potential of the cell interferes neuromuscular function Symptoms: fatigue, weakness, ileus, rhabdomyolysis(<2.5mmol/L), flaccid paralysis with respiratory compromise(<2mmol/L) Cause Renal losses Extrarenal losses: vomiting, gastric tubes, diarrhea, high-output enteric/pancreatic fistulas Intracellular shifts from medications or hyperthyroidism : CHF on multiple drugs, diuretics Primary hyperaldosteronism, renin-secreting tumor
![Hypokalemia [K+] < 3.5mmol/L hyperpolarization of the resting potential of the cell interferes neuromuscular function.](http://slidesplayer.org/slide/12439177/74/images/11/Hypokalemia+%5BK%2B%5D+%3C+3.5mmol%2FL+hyperpolarization+of+the+resting+potential+of+the+cell+interferes+neuromuscular+function..jpg "Symptoms: fatigue, weakness, ileus, rhabdomyolysis(<2.5mmol/L), flaccid paralysis with respiratory compromise(<2mmol/L) Cause. Renal losses. Extrarenal losses: vomiting, gastric tubes, diarrhea, high-output enteric/pancreatic fistulas. Intracellular shifts from medications or hyperthyroidism. : CHF on multiple drugs, diuretics. Primary hyperaldosteronism, renin-secreting tumor.")
12
Hypokalemia Treatment K replacement by oral or IV route
Oral: 40~100 mEq/day, in 2~4 doses IV: rate 10~20mEq/hr– when infused higher than 10mEq/hr, cardiac monitoring Frequent monitoring is needed (the rate can be as high as 40mEq/hr) ∵hypokalemia represents large intracellular deficits replenishing total body levels may take days Cardiac disease, after cardiac surgery: corrected > 4mmol/L GI loss가 지속되는 경우, extraordinary replacement 필요함
 ∵hypokalemia represents large intracellular deficits replenishing total body levels may take days. Cardiac disease, after cardiac surgery: corrected > 4mmol/L. GI loss가 지속되는 경우, extraordinary replacement 필요함.")
13
Hypokalemia Magnesium: 같이 monitor
important cofactor for potassium uptake and maintenance of intracellular potassium levels, reduces the risk for arrhythmia Concurrent acidemia treated with K replacement, before pH is corrected by bicarbonate (산증이 교정되면 K이 더 떨어지므로.)
")
14
metabolic acidosis DM ketoacidosis
glucose ↑→glycolysis↓→oxylativephyosphorylation of ketoacid↓ pH↓, HCO3-↓, AG↑ Kussmaul respiration(rapid, large tidal volume) → PaCO2<20 Hyperglycemic osmotic diuresis : ECW↓, Na+↓, K+ ↓ Tx :insulin + fluid and balanced electrolyte (NS, half saline) + KCL Incomplicated ketoacidosis면bicarbonate주지않는다.
 → PaCO2<20. Hyperglycemic osmotic diuresis : ECW↓, Na+↓, K+ ↓ Tx :insulin + fluid and balanced electrolyte (NS, half saline) + KCL. Incomplicated ketoacidosis면bicarbonate주지않는다.")
16
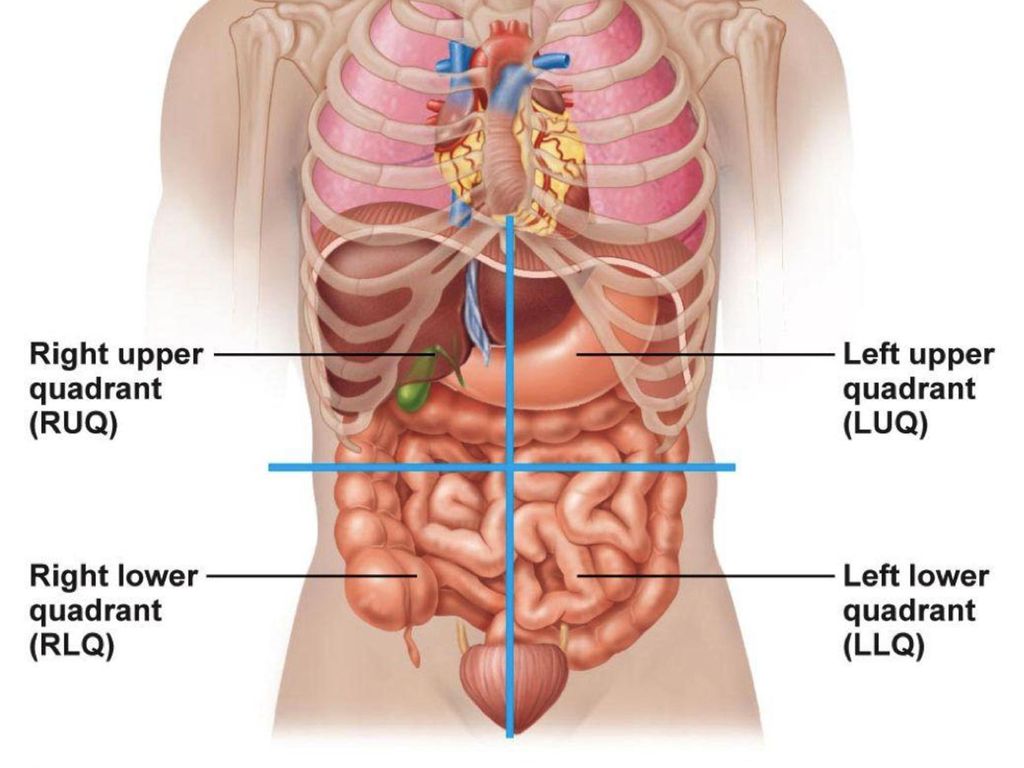
Pain cause RUQ LUQ RLQ pain LLQ acute cholecystitis acute cholangitis
GB stone hepatitis Rt. Ureter stone LUQ gastritis Lt. ureter stone Splenic infarction RLQ pain acute appendicitis Cecal diverticulitis ileocecal enteritis acute lymphadenitis LLQ D or sigmoid diverticulitis sigmoid volvulus colitis

17
Ureter stone 증상 진단 치료 갑작스런 극심한 복통 ( 옆구리 ) , 구역, 구토 소변검사 , CT , KUB
대증치료, 필요시 ESWL

Similar presentations




 란 ? 1) 넓은 의미 order 문서보고 2) 좁은 의미 ; 1 시간 검사실 검체 접수 문서보고.>")

 Cross contamination( 교차오염 ) Infected.>")
 주요 내용 소개>")






![MGR review 류마티스 내과 R4 최인아. [ 목차 ] Overlap syndrome (vs UCTD, MCTD) Polymyositis(PM) PM with Interstitial lung disease.](/42/11353284/big_thumb.jpg "MGR review 류마티스 내과 R4 최인아. [ 목차 ] Overlap syndrome (vs UCTD, MCTD) Polymyositis(PM) PM with Interstitial lung disease.>")




