Download presentation
1
요양병원내 노인성 폐렴 전남대병원 노년내과/호흡기내과 김유일

2
Contents 환자 특성/임상증상 원인균 진단 치료/예후 예방

3
Low BP, 80/40 (86.M) PH : Dementia, Parkinson’s ds, DM
PI : 요양병원 입원중, 아침 혈압 낮음 다음 검사는?

6
환자 특성 Kim et al. 요양병원에 입원 중인 환자에서 발생한 폐렴.
J Korean Geriatr Soc 2015;19(2):80-88
:")
7
Risk Factors for Aspiration
the elderly neurologic dysphagia stroke, neuromuscular ds abnormalities of the upper airway or GI tract gastroesophageal reflux (GERD), tracheoesophageal fistula drug/alcohol Poor oral- dental hygiene resulting in oropharyngeal colonization by respiratory tract pathogens, including Enterobacteriaceae, Pseudomonas aeruginosa, Staphylococcus aureus a supine position, gastroparesis, NG tube Especially in ICU patients
, tracheoesophageal fistula. drug/alcohol. Poor oral- dental hygiene. resulting in oropharyngeal colonization by respiratory tract pathogens, including Enterobacteriaceae, Pseudomonas aeruginosa, Staphylococcus aureus. a supine position, gastroparesis, NG tube. Especially in ICU patients.")
8
Location of apiration pn
FIGURE 98-1 Relationship between posture and location of lung abscess. With patient lying face up (A), aspiration occurs into the superior segment of the lower lobe. With patient lying on the side (B), aspiration occurs into the posterior segment of the upper lobe. (From Brock RC: Lung Abscess. Oxford, Blackwell, 1952.)
, aspiration occurs into the superior segment of the lower lobe. With patient lying on the side (B), aspiration occurs into the posterior segment of the upper lobe. (From Brock RC: Lung Abscess. Oxford, Blackwell, 1952.)")
10
증상 Kim et al. 요양병원에 입원 중인 환자에서 발생한 폐렴.
J Korean Geriatr Soc 2015;19(2):80-88
:")
11
검사실 결과 Kim et al. 요양병원에 입원 중인 환자에서 발생한 폐렴.
J Korean Geriatr Soc 2015;19(2):80-88
:")
12
Tx: Piperacillin & tazobactam + levofloxacin

13
원인균 : Pathogens for HCAP
Healthcare-associated pneumonia among hospitalized patients in a Korean tertiary hospital. -BMC Infectious Diseases :61

14
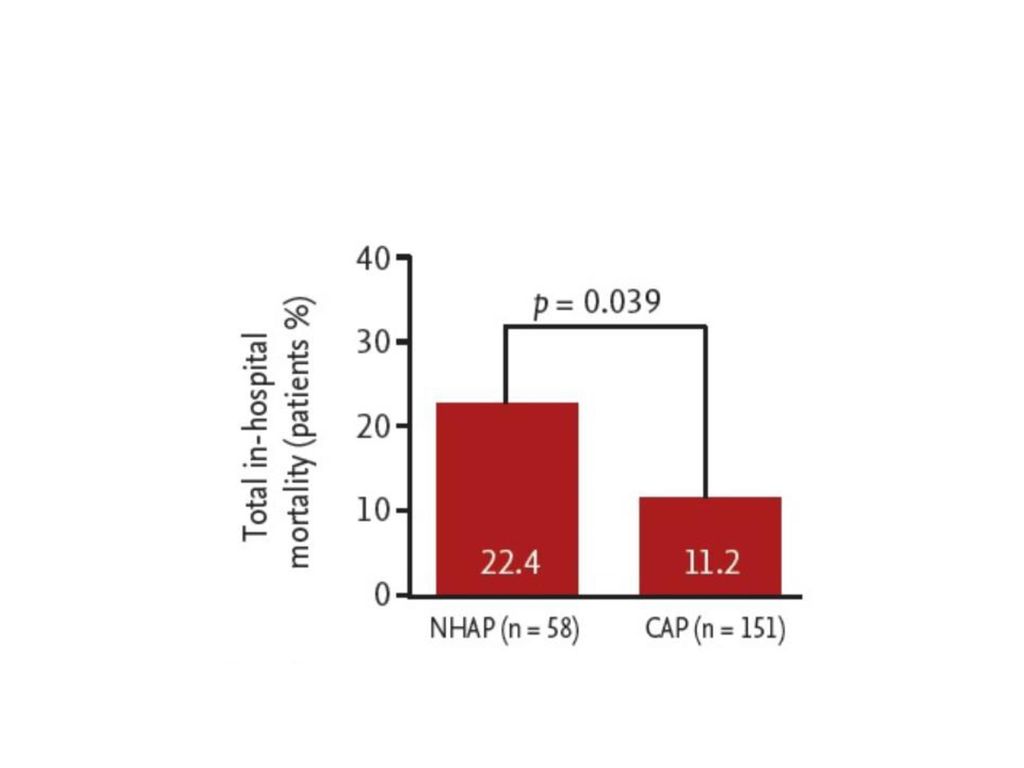
Microorganisms identified in elderly patients with pneumonia
- Koh et al. Clinical characteristics of nursing home-acquired pneumonia in elderly patients admitted to a Korean teaching hospital. Korean J Intern Med Sep; 30(5): 638–647.
: 638–647.")
15
Microbiology (흡인성 폐렴) mixed infection Outpatient (CAP) Inpatient (HAP)
aerobic + anaerobic/microaerophilic (Bacteroides, Fusobacterium) d/t oropharyngeal secretion aspiration Outpatient (CAP) S. pneumoniae, H. influenzae, S. aureus Inpatient (HAP) GNB, Pseudomonas aeruginosa, S. aureus
 d/t oropharyngeal secretion aspiration. Outpatient (CAP) S. pneumoniae, H. influenzae, S. aureus. Inpatient (HAP) GNB, Pseudomonas aeruginosa, S. aureus.")
16
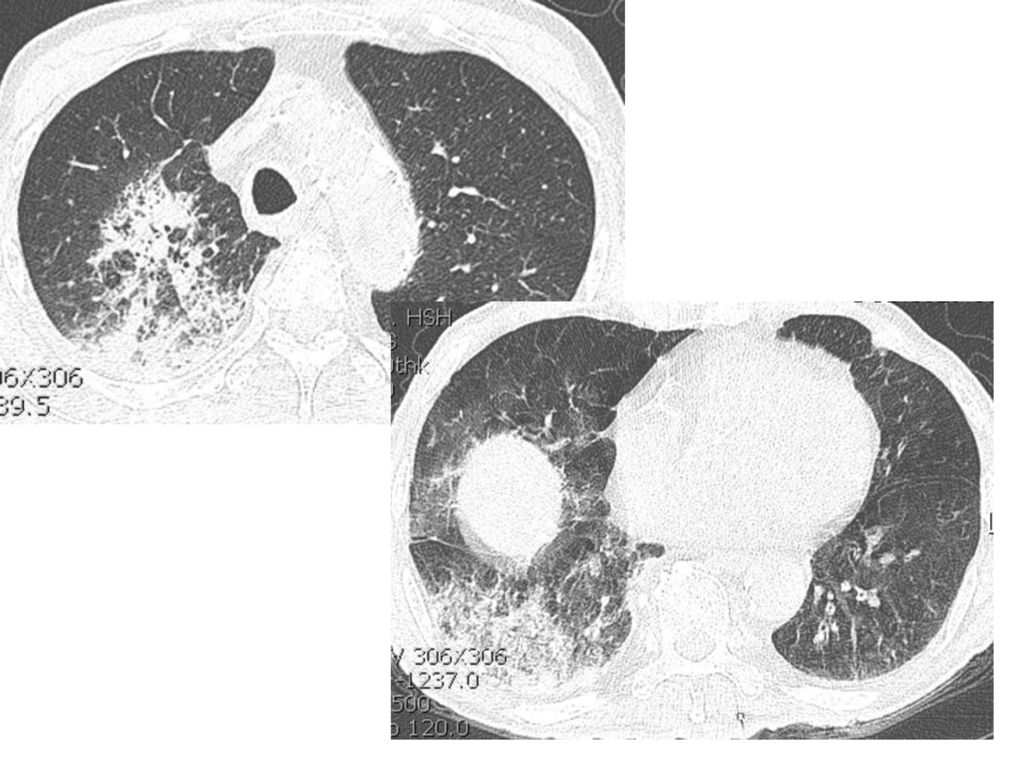
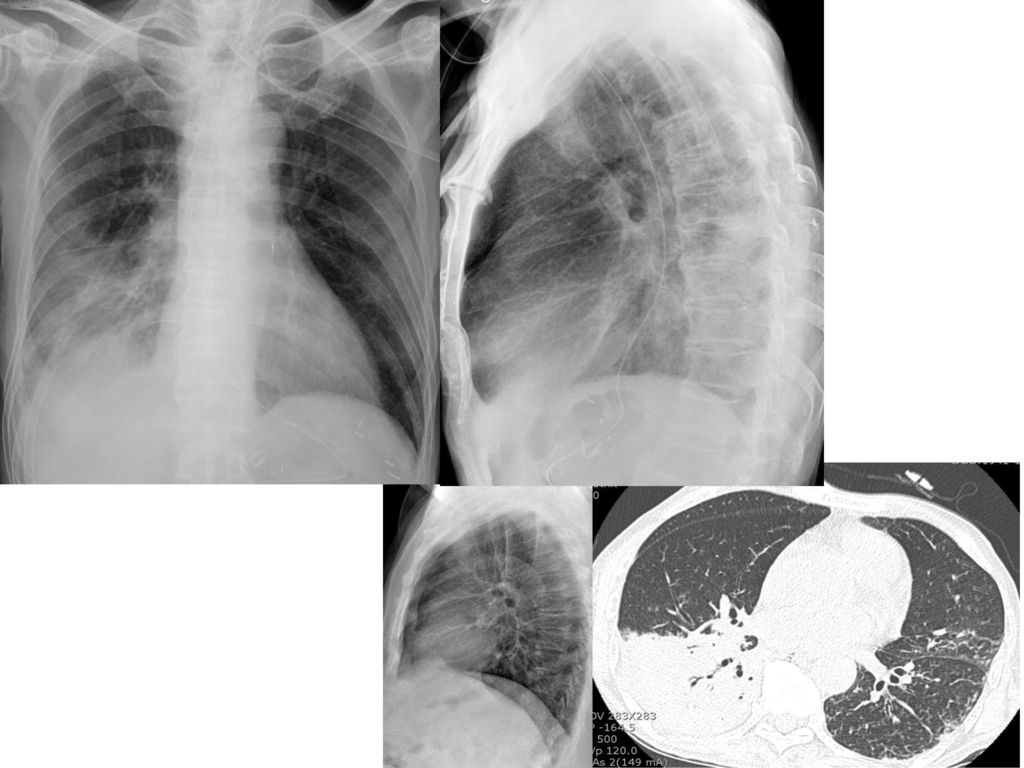
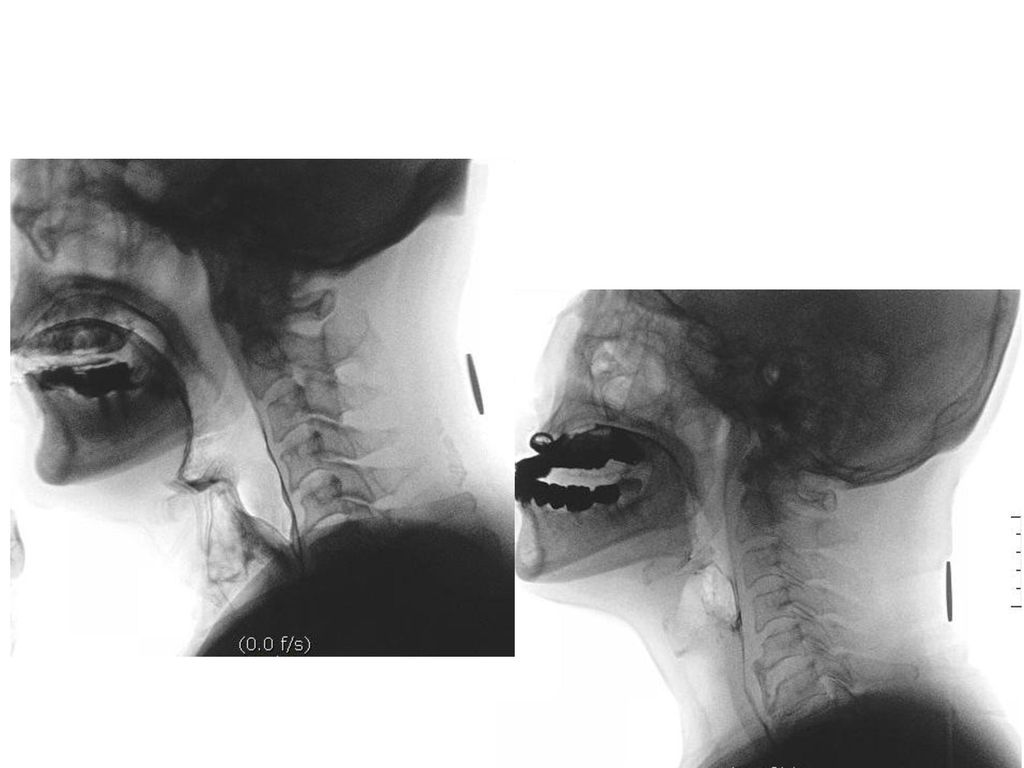
진단 (esp, 흡인성 폐렴) a high clinical index of suspicion. Chest X-ray
: (recurrent) bacterial pneumonia c risk factors Chest X-ray Involve on dependent area (호발 부위) ; posterior segment of upper lobe superior segment of lower lobe Sputum/tracheal secretions/ bronchoscopic sampling Tracheal secretions: lipid-laden macrophages , glucose level Cineradiographic swallowing studies VFSS (videofluoroscopic swallowing study, 비디오 연하조영검사) Others Tube feeding c methylene blue Radionuclide imaging studies Overnight esophageal pH monitoring
 bacterial pneumonia c risk factors. Chest X-ray. Involve on dependent area (호발 부위) ; posterior segment of upper lobe. superior segment of lower lobe. Sputum/tracheal secretions/ bronchoscopic sampling. Tracheal secretions: lipid-laden macrophages , glucose level. Cineradiographic swallowing studies. VFSS (videofluoroscopic swallowing study, 비디오 연하조영검사) Others. Tube feeding c methylene blue. Radionuclide imaging studies. Overnight esophageal pH monitoring.")
17
Initial antibiotic treatment in elderly patients admitted with pneumonia

18
TREATMENT Most initial therapy for HAP is empirical
major factor for antibiotics selection; risk factors for MDR pathogen Risk for MRSA; vancomycin, linezolid Similar to CAP with pseudomonas risk (except macrolide)
")
19
Treatment of HCAP (Harrison)
Patients without Risk Factors for MDR Pathogens Ceftriaxone (2 g IV q24h) or Moxifloxacin (400 mg IV q24h), ciprofloxacin (400 mg IV q8h), or levofloxacin (750 mg IV q24h) or Ampicillin/sulbactam (3 g IV q6h) or Ertapenem (1 g IV q24h) Patients with Risk Factors for MDR Pathogens 1. Beta-lactam: Ceftazidime (2 g IV q8h) or cefepime (2 g IV q8–12h) or Piperacillin/tazobactam (4.5 g IV q6h), imipenem (500 mg IV q6h or 1 g IV q8h), or meropenem (1 g IV q8h) plus 2. A second agent active against gram-negative bacterial pathogens: Gentamicin or tobramycin (7 mg/kg IV q24h) or amikacin (20 mg/kg IV q24h) or Ciprofloxacin (400 mg IV q8h) or levofloxacin (750 mg IV q24h) plus 3. An agent active against gram-positive bacterial pathogens: Linezolid (600 mg IV q12h) or Vancomycin (15 mg/kg, up to 1 g IV, q12h) Abbreviation: MDR, multidrug-resistant.
 or. Moxifloxacin (400 mg IV q24h), ciprofloxacin (400 mg IV q8h), or levofloxacin (750 mg IV q24h) or. Ampicillin/sulbactam (3 g IV q6h) or. Ertapenem (1 g IV q24h) Patients with Risk Factors for MDR Pathogens. 1. Beta-lactam: Ceftazidime (2 g IV q8h) or cefepime (2 g IV q8–12h) or. Piperacillin/tazobactam (4.5 g IV q6h), imipenem (500 mg IV q6h or 1 g IV q8h), or meropenem (1 g IV q8h) plus. 2. A second agent active against gram-negative bacterial pathogens: Gentamicin or tobramycin (7 mg/kg IV q24h) or amikacin (20 mg/kg IV q24h) or. Ciprofloxacin (400 mg IV q8h) or levofloxacin (750 mg IV q24h) plus. 3. An agent active against gram-positive bacterial pathogens: Linezolid (600 mg IV q12h) or. Vancomycin (15 mg/kg, up to 1 g IV, q12h) Abbreviation: MDR, multidrug-resistant.")
20
Treatment of aspiration pn
Empirical Antibiotics covering anaerobes (5-10 days) B-lactam/b-lactamase inhibitor ampicillin-sulbactam, piperacillin-tazobactam, ticarcillin-clavulanate Carbapenem Imipenem, meropenem Clindamycin, metronidazole Fluoroquinolones Moxifloxacin Severe or HAP Combination Tx Surgical Tx for nutrition in pts with recurrent aspiration gastrostomy or jejunostomy feeding tube
 B-lactam/b-lactamase inhibitor. ampicillin-sulbactam, piperacillin-tazobactam, ticarcillin-clavulanate. Carbapenem. Imipenem, meropenem. Clindamycin, metronidazole. Fluoroquinolones. Moxifloxacin. Severe or HAP. Combination Tx. Surgical Tx for nutrition in pts with recurrent aspiration. gastrostomy or jejunostomy feeding tube.")
21
ATB Tx for etiologic organism

22
Fever (82. M) P/H : Dementia, Parkinson’s ds
 P/H : Dementia, Parkinson’s ds")
23
예후 인자

24
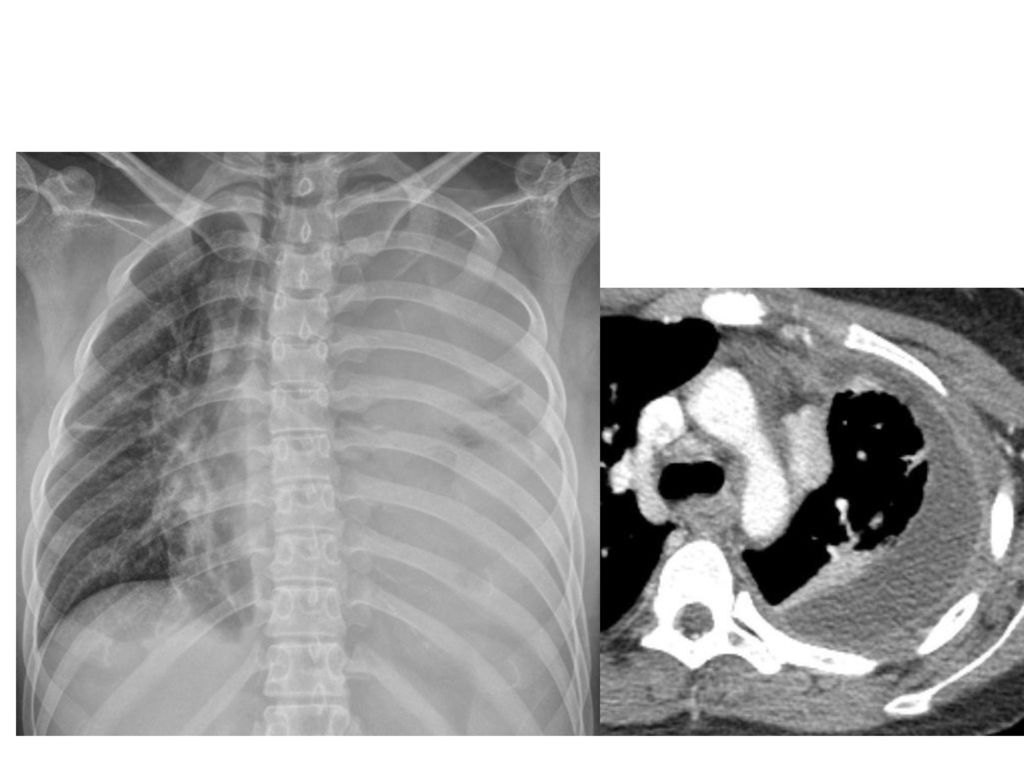
Cx & Px Empyema Px Most common, serious Cx Tx
Insertion of chest tubes Thoracotomy with decortication Px Comorbid condition 에 따른 영향 +

27
Sputum (60, M)
")
30
Prevention Pathogenic Mechanism Prevention Strategy
Oropharyngeal colonization with pathogenic bacteria Elimination of normal flora Avoidance of prolonged antibiotic courses Large-volume oropharyngeal aspiration around time of intubation Short course of prophylactic antibiotics for comatose patientsa Gastroesophageal reflux avoidance of high gastric residuals, prokinetic agents Bacterial overgrowth of stomach Prophylactic agents that raise gastric pHb Cross-infection from other colonized patients Hand washing, especially with alcohol-based hand rub; intensive infection control educationa; isolation; proper cleaning of reusable equipment Large-volume aspiration Endotracheal intubation; avoidance of sedation; decompression of small-bowel obstruction Microaspiration around endotracheal tube Endotracheal intubation Noninvasive ventilationa Prolonged duration of ventilation Daily awakening from sedation,a weaning protocolsa Abnormal swallowing function Early percutaneous tracheostomya Secretions pooled above endotracheal tube Head of bed elevateda; continuous aspiration of subglottic secretions with specialized endotracheal tubea; avoidance of reintubation; minimization of sedation and patient transport Altered lower respiratory host defenses Tight glycemic controlb; lowering of hemoglobin transfusion threshold; specialized enteral feeding formula aStrategies demonstrated to be effective in at least one randomized controlled trial. bStrategies with negative randomized trials or conflicting results.

31
Case (60세. M) C/C: 호흡곤란 악화 (D: 1 day ago-)
PI: 뇌경색증으로 중환자실 mechanical ventilator 치료 7일째 되는날 갑자기 호흡곤란 악화로, ventilator setting 상 산소요구량 (FiO2)가 증가되었다. Fever와 chills도 있었으며, tracheal secretions이 최근 많아졌다. P/E: Inspiratory crackles on both lower lung field (특히 등 부위에서 저명하게 들림). 양측 폐야의 호흡음 감소는 없음. Chest AP & CT는 다음과 같았다.
가 증가되었다. Fever와 chills도 있었으며, tracheal secretions이 최근 많아졌다. P/E: Inspiratory crackles on both lower lung field (특히 등 부위에서 저명하게 들림). 양측 폐야의 호흡음 감소는 없음. Chest AP & CT는 다음과 같았다.")
32
BT: 38.0℃ WBC 12,000/uL (Nu: 90%)
")
33
1. 가장 가능성 높은 진단명과 그 근거들은? 2. 이 환자에서 추가로 확인해야 할 사항들은 (추가 병력 청취 내용들은)? 3. 진단 및 원인 확인을 위해서 추가로 시행할 검사들은?

34
2. 이 환자에서 추가로 확인해야 할 사항들은 (추가 병력 청취 내용들은)?
1. 가장 가능성 높은 진단명과 그 근거들은? HCAP_aspiration pn (획득장소/병인), necrotizing pn or abscess_LUL resp sx (acute cough) with fever, inspiratory crackles_LULF, leukocytosis, infiltrates c necrosis at dependent segment Hospitalization Hx. <3mo 2. 이 환자에서 추가로 확인해야 할 사항들은 (추가 병력 청취 내용들은)? Risk Factors for Aspiration (neurologic ds, upper airway/GI ds, alcohol, drug, oral hygiene, combined ds 3. 진단 및 원인 확인을 위해서 추가로 시행할 검사들은? Sputum exam, VFSS, chest CT
, necrotizing pn or abscess_LUL. resp sx (acute cough) with fever, inspiratory crackles_LULF, leukocytosis, infiltrates c necrosis at dependent segment. Hospitalization Hx. <3mo. 2. 이 환자에서 추가로 확인해야 할 사항들은 (추가 병력 청취 내용들은) Risk Factors for Aspiration. (neurologic ds, upper airway/GI ds, alcohol, drug, oral hygiene, combined ds. 3. 진단 및 원인 확인을 위해서 추가로 시행할 검사들은 Sputum exam, VFSS, chest CT.")
35
요약 환자 특성/임상증상 원인균 진단 치료/예후 예방

36
Summary HCAP, Aspiration pneumonia Dependent area lesion Risk factors
Tx : antipseudomonal, anaerobic coverage



 Case 1.>")
 의 이해 흉부 기본 촬영 방사선 흉부 해부학 position of tubes and catheters.>")





 주요 내용 소개>")


 학회참석 및 연구 결과 발표)>")





>")


