Download presentation
1
MIC 법을 이용한 항생제 감수성 검사의 오류분석과 해결방법
성균관의대 삼성서울병원 진단검사의학과 이남용

2
목차 1 2 3 4 자동화 기기를 이용시 오류분석과 해결방법 항균제 선택보고시 오류분석과 해결방법
서론 2 항균제 선택보고시 오류분석과 해결방법 3 균종별, 항균제별 취약점 분석 4 자동화 기기를 이용시 오류분석과 해결방법

3
항균제 감수성 검사의 목적 특정 항균제에 대한 성공적 치료를 생체외 검사를 통하여 예견
감염 원인균에 대한 치료 효과가 높은 항균제를 선택 정기적 항생제 내성률 조사

4
Minimum Inhibitory Concentration (MIC)
The MIC is determined from the lowest concentration that exhibits inhibition of growth. The MIC may tell a physician the concentration of antimicrobial agent required at the site of infection to inhibit the infecting organism. Whenever MIC results are reported to clinicians to direct therapy, an interpretive category (ie, susceptible, intermediate, or resistant) should accompany the MIC result based on the criteria outlined in CLSI M100.
 should accompany the MIC result based on the criteria outlined in CLSI M100.")
5
However, the MIC does not represent an absolute value.
The ‘true’ MIC is somewhere between the lowest test concentration and the next lower test concentration. For example, 2-fold dilutions were used and the MIC is 16 μg/mL, the ‘true’ MIC would be between 16 μg/mL and 8 μg/mL. (e.g. MIC ≥ 16 μg/mL, MIC > 8 μg/mL) Even under the best of controlled conditions, a dilution test may not yield the same end point each time it is performed. Generally, the acceptable reproducibility of the test is within one twofold dilution of the actual end point. To avoid greater variability, the dilution test must be standardized and carefully controlled. CLSI M07-A9, 2012
 Even under the best of controlled conditions, a dilution. test may not yield the same end point each time it is. performed. Generally, the acceptable reproducibility of. the test is within one twofold dilution of the actual end point. To avoid greater variability, the dilution test must be. standardized and carefully controlled. CLSI M07-A9,")
6
1 항균제 선택보고시 오류분석과 해결방법 2 균종별, 항균제별 취약점 분석 3 자동화 기기를 이용시 오류분석과 해결방법

7
1. Selection of Antimicrobial Agents
균종과 항균제의 조합이 맞지 않는 항균제를 검사하지는 않는가? 균종별로 꼭 필요한 항균제 감수성 검사를 시행하는가? 보고하지 않아야 하는 항균제가 포함되어 있지 않은가? 소변검체에만 보고해야 되는 항균제를 다른 검체에서 보고하고 있지는 않는가?

11
예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 1차
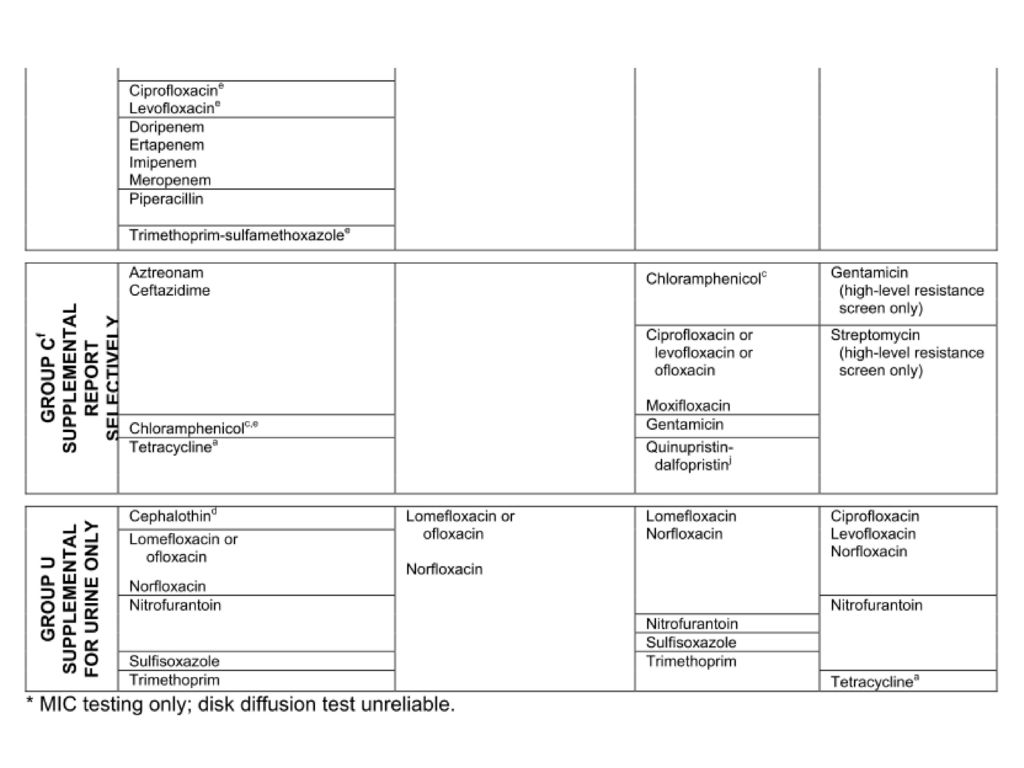
Enterococcus faecium (from positive blood culture) Warning (CLSI M100-S22, p37) Cephalosporin, aminoglysides (except for high-level resistance screeing), clindamycin, and trimethoprim-sulfamethoxazole may appear active in vitro, but are not effective clinically and should not be reported as susceptible. Enterococcus spp (CLSI M100-S22) Group A Ampicillin, Penicillin Group B Daptomycin Linezolid Vancomycin Group C Gentamicin (high-level resistance screen only) Streptomycin (high-level resistance screen only) Group U Ciprofloxacin, Levofloxacin, norfloxacin Nitrofurantoin Tetracycline vancomycin, teicoplanin에 고도내성인 전형적인 반코마이신 내성 E. faecium입니다. Enterococcus spp.는 내재적인 항균제 내성이 많고, vancomycin 내성률이 높아서 감수성 검사를 실시하는 항균제를 적절하게 선택하는 것이 중요. Penicillin, ampicillin이 가장 기본적인 항균제이고, daptomycin, linezolid, synercid (O), vancomycin 이 이차적인 항균제, ciprofloxacin 등의 퀴놀론, nitrofurantoin, tetracycline은 소변 분리주에만 감수성 검사를 권장. Cephalosporin, AG, clindamycin, EM, Bactrim등에는 내인성 내성이므로 감수성 검사를 하지 않아야함. 소변분리주에만 보고되어야 하는 levofloxacin 등 fluoroquinolone계 항균제를 혈액배양이라는 검체 조건을 고려하지 않고 보고한 기관들이 수십 곳에 달했습니다. 이들 기관은 장구균에 대한 항균제감수성 패널구성과 보고범위를 검토해야 할 것으로 생각합니다. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 1차
 Warning (CLSI M100-S22, p37) Cephalosporin, aminoglysides (except for high-level resistance screeing), clindamycin, and trimethoprim-sulfamethoxazole may appear active in vitro, but are not effective clinically and should not be reported as susceptible. Enterococcus spp (CLSI M100-S22) Group A. Ampicillin, Penicillin. Group B. Daptomycin. Linezolid. Vancomycin. Group C. Gentamicin (high-level resistance screen only) Streptomycin (high-level resistance screen only) Group U. Ciprofloxacin, Levofloxacin, norfloxacin. Nitrofurantoin. Tetracycline. vancomycin, teicoplanin에 고도내성인 전형적인 반코마이신 내성 E. faecium입니다. Enterococcus spp.는 내재적인 항균제 내성이 많고, vancomycin 내성률이 높아서 감수성 검사를 실시하는 항균제를 적절하게 선택하는 것이 중요. Penicillin, ampicillin이 가장 기본적인 항균제이고, daptomycin, linezolid, synercid (O), vancomycin 이 이차적인 항균제, ciprofloxacin 등의 퀴놀론, nitrofurantoin, tetracycline은 소변 분리주에만 감수성 검사를 권장. Cephalosporin, AG, clindamycin, EM, Bactrim등에는 내인성 내성이므로 감수성 검사를 하지 않아야함. 소변분리주에만 보고되어야 하는 levofloxacin 등 fluoroquinolone계 항균제를 혈액배양이라는 검체 조건을 고려하지 않고 보고한 기관들이 수십 곳에 달했습니다. 이들 기관은 장구균에 대한 항균제감수성 패널구성과 보고범위를 검토해야 할 것으로 생각합니다. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 1차.")
12
예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 1차
Stenotrophomonas maltophilia Naturally resistant to many broad-spectrum antibiotics (including all carbapenems) Stenotrophomonas maltophilia (CLSI M100-S22) Group A Trimethoprim-sulfamethoxazole Group B *Ceftazidime *Chloramphenicol Levofloxacin Minocycline *Ticarcillin-clavulanate *MIC testing only. S. maltophilia는 oxidase 양성 비발효 그람음성간균으로 내인성 다제내성균인데, 감수성검사의 정확도가 떨어지기 때문에 많은 항균제 종류에 대해 감수성검사를 하지 않도록 제한되어 있음을 주의해야 합니다. CLSI 지침에 의하면 디스크확산법으로 감수성검사를 할 수 있는 약제는 ceftazidime, minocycline, levofloxacin, trimethoprime-sulfamethoxazole에 불과합니다. 앞의 항균제감수성결과 통계에서 보듯이 부적절한 항균제에 대해 감수성결과를 보고함으로써 감점을 받는 경우가 빈번하였습니다. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 1차
 Stenotrophomonas maltophilia. (CLSI M100-S22) Group A. Trimethoprim-sulfamethoxazole. Group B. *Ceftazidime. *Chloramphenicol. Levofloxacin. Minocycline. *Ticarcillin-clavulanate. *MIC testing only. S. maltophilia는 oxidase 양성 비발효 그람음성간균으로 내인성 다제내성균인데, 감수성검사의 정확도가 떨어지기 때문에 많은 항균제 종류에 대해 감수성검사를 하지 않도록 제한되어 있음을 주의해야 합니다. CLSI 지침에 의하면 디스크확산법으로 감수성검사를 할 수 있는 약제는 ceftazidime, minocycline, levofloxacin, trimethoprime-sulfamethoxazole에 불과합니다. 앞의 항균제감수성결과 통계에서 보듯이 부적절한 항균제에 대해 감수성결과를 보고함으로써 감점을 받는 경우가 빈번하였습니다. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 1차.")
13
Strepcococcus pneumoniae
S. pneumoniae 감수성 검사에서 penicillin, cephalosporin, meropenem 감수성 검사에 여전히 디스크 확산법으로 검사하여 결과를 제출하는 것은 문제점. 하지만, 1ug oxacillin 디스크로 대신 디스크확산법 검사를 해서 억제대가 20mm 이상이면 MIC를 0.06 ug/mL으로 판정할 수 있고, 억제대가 19mm 이하면 직접 MIC를 구해야 한다. 디스크 확산법에서 penicillin, cephalosporin, meropenem 디스크등을 사용하여 감수성 검사를 한 기관은 감점 요인이다. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 2차
 대한임상검사정도관리협회 임상미생물학분과 정도관리 2011년 2차.")
14
Strepcococcus pneumoniae

15
S. pneumoniae Oxacillin disk diffusion testing Result
Disk Participants Antimicrobials # S I R % Acceptiable Zone diameters mean Oxacillin 72 1 - 71 6.8 MIC Participants 모두 Inappropriate response Antimicrobials # S I R % Acceptiable Oxacillin 4 - An oxacillin disk diffusion test can be used as a surrogate for detecting penicillin susceptibility. Disk diffusion testing using the standard 10 unit penicillin disk is not reliable for pneumococci. If the oxciilin zone measures >=20 mm, the isolate can be reported as penicillin susceptible (MIC =<0.06). Penicillin and cefotaxime, ceftriaxone, or meropenem MICs should be determined for those isolates with oxacillin zone diameters of <=19 mm, because zones of <= 19mm occur with penicillin-resistant, intermediate, or certain susceptible strains (CLSI M100-S22 p105). Oxacillin should never be reported and isolates with oxacillin zones 19 mm or less must be subjected to a penicillin MIC before reporting peniciilin results. Any oxacillin result reported was considered an inappropriate response in this Survey. Over 98% of laboratories reported results from the oxacillin screen for penicillin susceptibility correctly as ‘Possibly resistant, MIC testing required for confirmation’ (CAP 분석내용) Oxacillin disk test can be used as a surrogate for detecting penicillin susceptibility. Oxacillin should never be reported and isolates with zones 19 mm or less must be subjected to a penicillin MIC before reporting penicillin results. ‘Possibly resistant, MIC testing required for confirmation’ 예시) CAP survey Bacteriology 2010, D-B
. Penicillin and cefotaxime, ceftriaxone, or meropenem MICs should be determined for those isolates with oxacillin zone diameters of <=19 mm, because zones of <= 19mm occur with penicillin-resistant, intermediate, or certain susceptible strains (CLSI M100-S22 p105). Oxacillin should never be reported and isolates with oxacillin zones 19 mm or less must be subjected to a penicillin MIC before reporting peniciilin results. Any oxacillin result reported was considered an inappropriate response in this Survey. Over 98% of laboratories reported results from the oxacillin screen for penicillin susceptibility correctly as ‘Possibly resistant, MIC testing required for confirmation’ (CAP 분석내용) Oxacillin disk test can be used as a surrogate for detecting penicillin susceptibility. Oxacillin should never be reported and isolates with zones 19 mm or less must. be subjected to a penicillin MIC before reporting penicillin results. ‘Possibly resistant, MIC testing required for confirmation’ 예시) CAP survey Bacteriology 2010, D-B.")
16
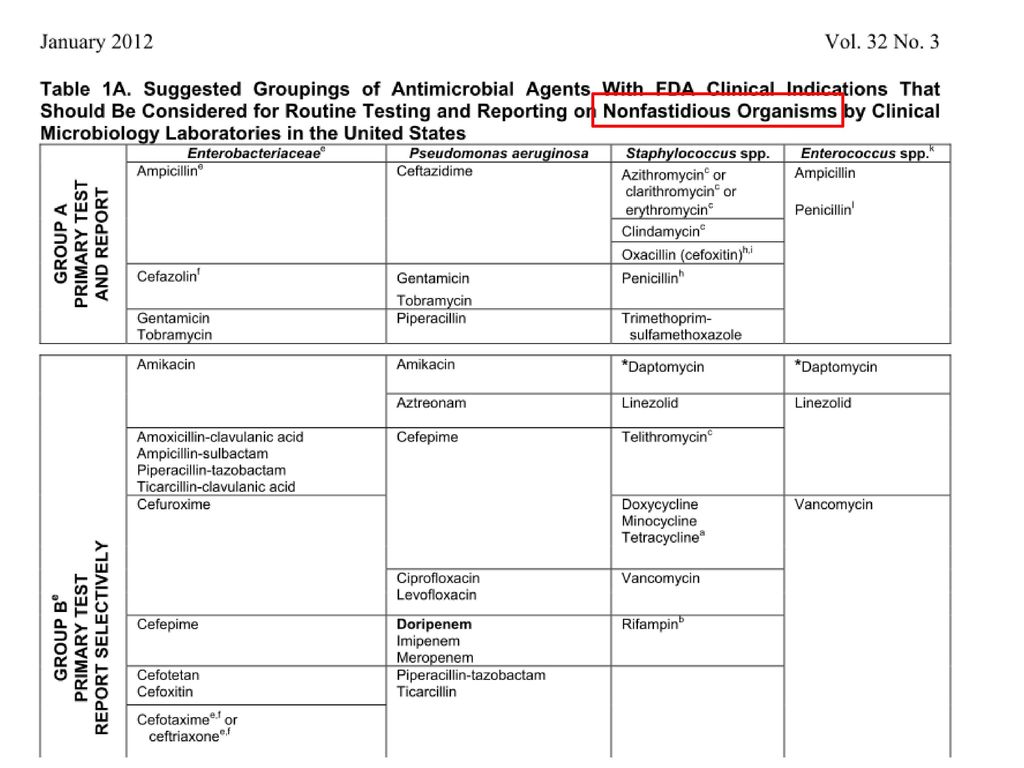
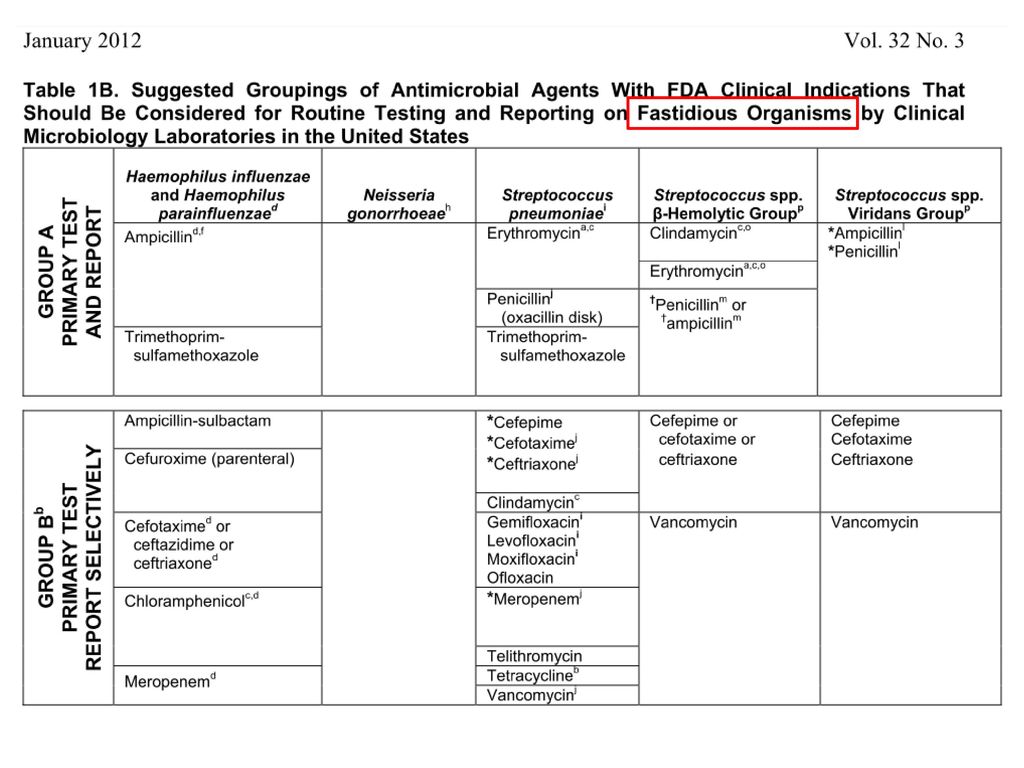
Guidelines for selection of appropriate Antimicrobial agents
To make routine susceptibility testing relevant and practical, the number of agents tested should be limited. CLSI M100 Tables 1A to 1C lists those agents that fulfill the basic requirements for routine use in most clinical laboratories. These guidelines are based on drugs with clinical indications approved by the US Food and Drug Administration (FDA) in the United States. - Agents may be added to or removed from these basic lists as conditions demand. In other countries, placement of antimicrobial agents in Tables 1A and 1B should be based on available drugs approved for clinical use by relevant regulatory agentics.
 in the United States. - Agents may be added to or removed from these basic lists as conditions demand. In other countries, placement of antimicrobial agents in Tables 1A and 1B should be based on available drugs approved for clinical use by relevant regulatory agentics.")
21
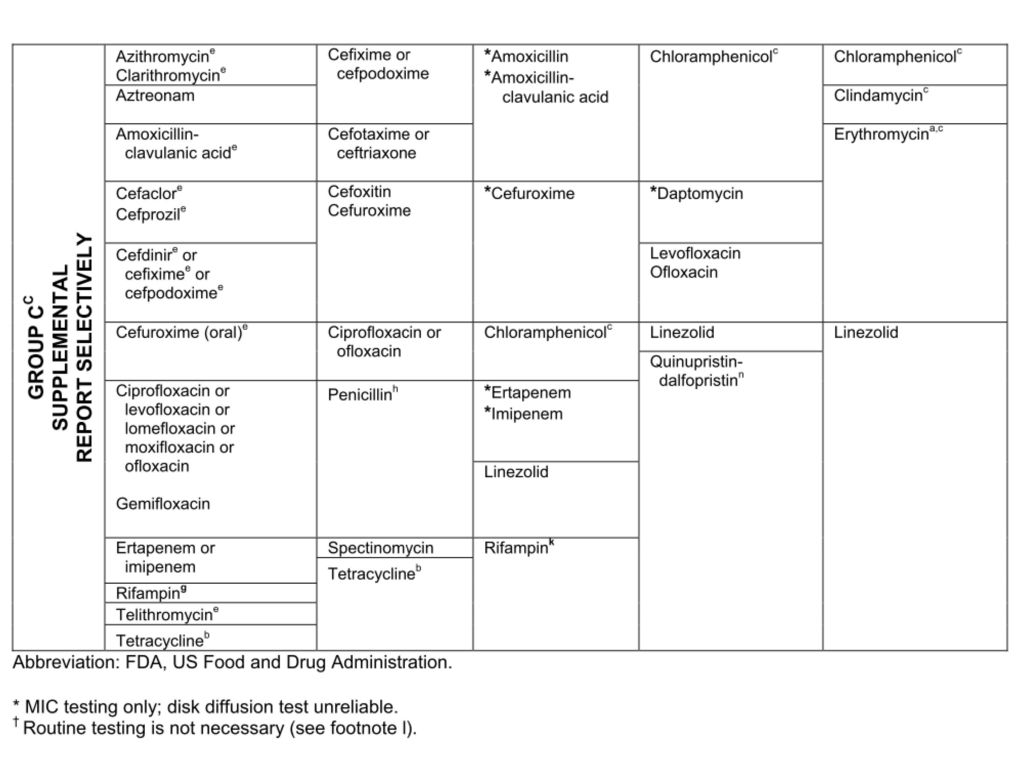
Test/Report Groups Group A: primary test and report
Group B: primary test, report selectively Group C: supplemental report selectively Group U (Urine): antimicrobial agents that are used only or primarily for treating urinary tract infections. Group O (Other): clinical indication, not candidate for routine testing in USA Group Inv. (Investigational): not approved by FDA
: antimicrobial agents that are used only or primarily for treating urinary tract infections. Group O (Other): clinical indication, not candidate for routine testing in USA. Group Inv. (Investigational): not approved by FDA.")
22
Drugs listed together in a single box are agents for which interpretive results (susceptible, intermediate, or resistant) and clinical efficacy are similar. Results from one agent connected by an ‘or’ can be used to predict results for the other agent. When no ‘or’ connects agents within a box: testing of one agent cannot be used to predict results for another.

23
Selective Testing and Reporting
Each laboratory should decide which agents in M100 Tables 1A, 1B and 1C to report routinely (Group A) and which might be reported only selectively (Group B). Of results for Group B agents - Unexpected resistance, when confirmed, should be reported. (eg, resistance to a secondary agent but susceptibility to a primary agent)
 and which might be reported only selectively (Group B). Of results for Group B agents. - Unexpected resistance, when confirmed, should be reported. (eg, resistance to a secondary agent but susceptibility to a primary agent)")
24
*MIC testing only Reliable disk diffusion susceptibility tests with agents do not yet exist. S. pneumoniae Penicillin and cefotaxime, ceftriaxone or meropenem should be tested by a reliable MIC method. Pneumococcus There are several beta-lactam agents that might be used for treating pneumococcal infections that cannot be reliably tested by the disk diffusion method and there are no disk diffusion breakpoints for these agents. These include amoxicillin, ampicillin, cefepime, cefotaxime, ceftriaxone, cefuroxime, ertapenem, imipenem, and meropenem. Consequently, an MIC method must be used for testing these agents. Neiseria meningitidis Penicillin / ampicillin Disk diffusion tests with ampicillin and penicillin are unreliable for N. meningitidis. MIC tests should be used for this organism

25
1 항균제 선택보고시 오류분석과 해결방법 2 균종별, 항균제별 취약점 분석 3 자동화 기기를 이용시 오류분석과 해결방법

26
균종별/항균제별 취약점 Penicillin and ampicillin MICs with β-lactamase
: Broth and agar dilution tests may not accurately detect Penicillin and Ampicillin resistance with β-lactamase producing CNS and enterococci strains. S. aureus with penicillin MICs ≤ 0.12 μg/mL or zone diameters ≥ 29mm Nitrocefin-based tests or penicillin disk diffusion zone-edge test Enterococci with penicillin and ampicillin resistance Because of production of low-affinity, PBPs or rarely β-lactamase Resistance in these strains is best detected by using a direct nitrocefin-based β-lactamase test. CLSI guide M07-A9 p.23 < Staphylococcis > Staphylococcal beta-lactamase is readily inducible, there is a risk of this occurring if penicillin were used to treat such strains. For this reason it is recommended that isolates of Staphylococcus with penicillin MICs <=0.12 ug/mL or zone diameters >=29 mm be tested for beta-lactamase production before reporting the isolate as penicillin susceptible. These include nitrocefin-based tests or evaluating the zone edge of a penicillin disk diffusion test. The penicillin disk diffusion zone-edge test was more sensitive than nitrocefin-based tests for detection of beta-lactamase production in S. aureus. Sharp(cliff) – positive (R), Fuzzy(beach) – negative (S) CLSI guide M07-A9 p.28 < Enterococci > A positive β-lactamase test predicts resistance to penicillin, and amino-, carboxy- and ureidopenicillins. CLSI M07-A9, 2012
 – positive (R), Fuzzy(beach) – negative (S) CLSI guide M07-A9 p.28 < Enterococci > A positive β-lactamase test predicts resistance to penicillin, and amino-, carboxy- and ureidopenicillins. CLSI M07-A9,")
27
균종별/항균제별 취약점 Clindamycin
: 유도성 MLSb 내성기전에 의한 clindamycin 내성 S. aureus 검체 : 통상적인 감수성검사에서는 감수성이나 , 국내 S. aureus는 대부분 inducible clindamycin 내성이므로 이를 확인하는 검사가 필요. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2010년 2차
 대한임상검사정도관리협회 임상미생물학분과 정도관리 2010년 2차.")
28
Clindamycin : 상용화된 희석법을 사용하는 기관에서는 Erythromycin과
clindamycin 이 함유된 well을 한 개 추가함으로써 inducible clindamycin 내성검사결과를 확인가능함. Single well with 4 μg/mL Erythromycin + 0.5 μg/mL Clindamycin (4/0.5) AST rule will automatically change the Clindamycin interpretation to R* when Erythromycin is I or R, and Clindamycin is S or I, and the inducible Clindamycin test is positive. 디스크확산법을 사용하는 기관은 erythromycin과 clindamycin을 근접시켜 배치하면 D-zone 검사를 감수성검사와 동시에 실시할 수 있고, 상용화된 희석법을 사용하는 기관에서는 erythromycin과 clindamycin이 함유된 well이 한 개 추가되면 감수성검사를 하는 과정에서 inducible clindamycin 내성검사결과를 확인할 수 있습니다. Icd : Inducibla Cindamycin
 AST rule will automatically change the. Clindamycin interpretation to R* when. Erythromycin is I or R, and Clindamycin. is S or I, and the inducible Clindamycin. test is positive. 디스크확산법을 사용하는 기관은 erythromycin과 clindamycin을 근접시켜 배치하면 D-zone 검사를 감수성검사와 동시에 실시할 수 있고, 상용화된 희석법을 사용하는 기관에서는 erythromycin과 clindamycin이 함유된 well이 한 개 추가되면 감수성검사를 하는 과정에서 inducible clindamycin 내성검사결과를 확인할 수 있습니다. Icd : Inducibla Cindamycin.")
29
균종별/항균제별 취약점 Vancomycin
: Vancomycin은 디스크확산법은 권장되지 않고, teicoplanin 감수성 검사 기준도 정립되지 않음. 반드시 확인검사가 필요함. 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2010년 2차
 대한임상검사정도관리협회 임상미생물학분과 정도관리 2010년 2차.")
30
Vancomycin MIC (μg/mL ) Vancomycin Agar Screen
: S. aureus with vancomycin MICs ≥ 32 μg/mL can be detected by either MIC, disk diffusion, or the vancomycin agar screen test. However, strains with vancomycin MICs < 32 μg/mL are not detected by disk diffusion, even with 24-hour incubation. < Ability of Various Methods to detect levels of Vancomycin Susceptibility in S. aureus > Vancomycin MIC (μg/mL ) MIC Method Disk Diffusion Method Vancomycin Agar Screen <=2 (S) Yes No 4 (I) Variable 8 (I) 16 (R) >=32 (R) In order to recognize strains of staphylococci for which the vancomycin MICs are 4 to 16, MIC testing must be performed and the tests incubated for a full 24 hours at 35+/-2 C. Strains with vancomycin MICs <32 are not detected by disk diffusion, even with 24-hour incubation. The vancomycin agar screen test may be used to detec isolates of S. aureus with vancomycin MIC >=8; however, this medium does not consistently detect S. aureus with vancomycin MICs of 4. Until further data on the prevalence of clinical significance of isolates with reduced susceptibility to vancomycin are known, laboratories my choose to examine MRSA strains more carefully for elevated MICs to vancomycin. ( CLSI guideline M02-A11, 2012 p.21) CLSI guideline M02-A11, 2012
 MIC Method. Disk Diffusion Method. Vancomycin Agar Screen. <=2 (S) Yes. No. 4 (I) Variable. 8 (I) 16 (R) >=32 (R) In order to recognize strains of staphylococci for which the vancomycin MICs are 4 to 16, MIC testing must be performed and the tests incubated for a full 24 hours at 35+/-2 C. Strains with vancomycin MICs <32 are not detected by disk diffusion, even with 24-hour incubation. The vancomycin agar screen test may be used to detec isolates of S. aureus with vancomycin MIC >=8; however, this medium does not consistently detect S. aureus with vancomycin MICs of 4. Until further data on the prevalence of clinical significance of isolates with reduced susceptibility to vancomycin are known, laboratories my choose to examine MRSA strains more carefully for elevated MICs to vancomycin. ( CLSI guideline M02-A11, 2012 p.21) CLSI guideline M02-A11,")
31
균종별/항균제별 취약점 Enterobacteriaceae – cephalosporin breakpoint
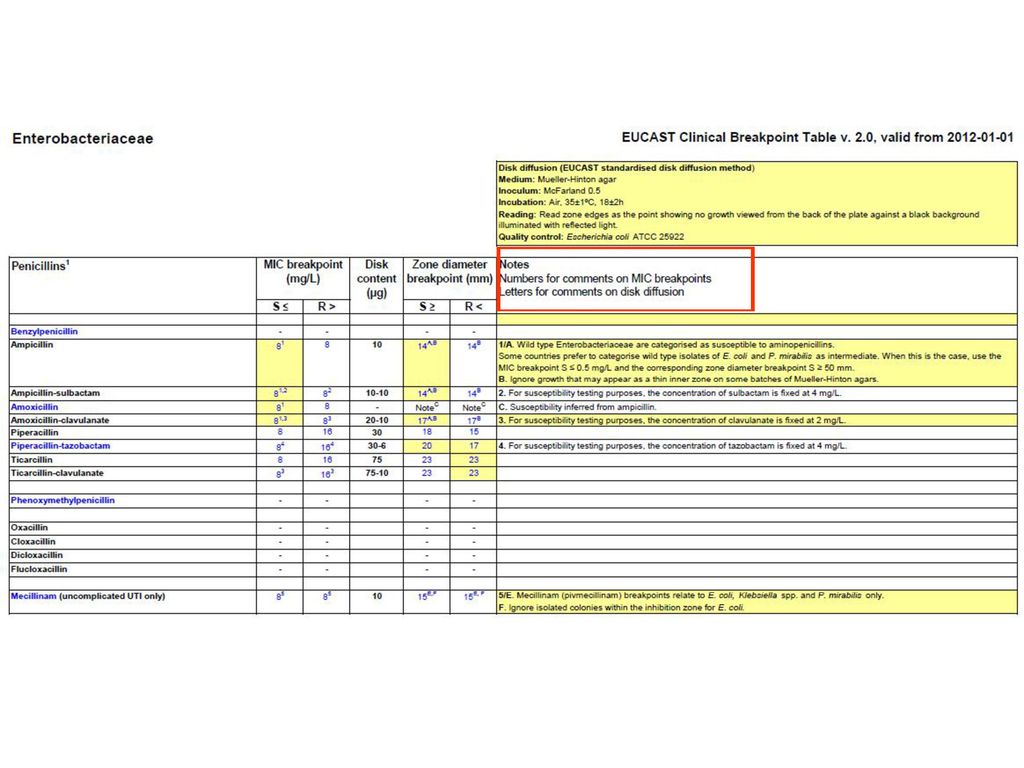
When using the current criteria, routine ESBL testing is no longer necessary before reporting results. Antimicrobials CLSI M100-S19 (ug/ml) CLSI M100-S20 CLSI M100-S22 S I R Cefazolin <=8 16 >=32 <=1 2 >=4 <=2 4 >=8 Cefotaxime 16-32 >=64 Ceftriaxone Ceftazidime <=4 8 >=16 Ceftizoxime Cefepime Cefoxitin 2010년 CLSI는 ESBL 확인검사없이 통상적인 감수성 검사만으로 결과를 보고할 수 있도록 Enterobacteriaceae 의 cephalosporin 의 감수성 판독기준을 낮추었다. 하지만, CLSI는 cefazolin, cetrazidime, cetfriaxone, cefotaxime, cetrizoxime 의 기준을 바꾼 것과는 달리 4세대 cephalosporin 인 cefepime과 cephamycin인 cefoxitin의 감수성 판독기준은 이전과 동일하게 유지하였다. 이는 유럽의 항균제감수성 검사기준을 제공하는 EUCAST 가 cefepime의 감수성 판독기준을 <1로 제시하고 있는 것과는 다른 점으로 CLSI에서 cefepime의 감수성 판독기준을 낮추지 않은 것은 기준을 낮추면 ESBL이 아닌 AmpC등에 의해 cephalosporin 내성을 획득한 균주들이 cefepime에도 내성으로 판독되는 오류때문이다. 그러나 cefepime의 판독기준은 동일하게 유지됨.
 CLSI M100-S20. CLSI M100-S22. S. I. R. Cefazolin. <= >=32. <=1. 2. >=4. <=2. 4. >=8. Cefotaxime >=64. Ceftriaxone. Ceftazidime. <=4. 8. >=16. Ceftizoxime. Cefepime. Cefoxitin. 2010년 CLSI는 ESBL 확인검사없이 통상적인 감수성 검사만으로 결과를 보고할 수 있도록 Enterobacteriaceae 의 cephalosporin 의 감수성 판독기준을 낮추었다. 하지만, CLSI는 cefazolin, cetrazidime, cetfriaxone, cefotaxime, cetrizoxime 의 기준을 바꾼 것과는 달리 4세대 cephalosporin 인 cefepime과 cephamycin인 cefoxitin의 감수성 판독기준은 이전과 동일하게 유지하였다. 이는 유럽의 항균제감수성 검사기준을 제공하는 EUCAST 가 cefepime의 감수성 판독기준을 <1로 제시하고 있는 것과는 다른 점으로 CLSI에서 cefepime의 감수성 판독기준을 낮추지 않은 것은 기준을 낮추면 ESBL이 아닌 AmpC등에 의해 cephalosporin 내성을 획득한 균주들이 cefepime에도 내성으로 판독되는 오류때문이다. 그러나 cefepime의 판독기준은 동일하게 유지됨.")
32
Enterobacteriaceae – cephalosporin breakpoint
: ESBL의 경우 감수성인 cephalosporin 결과를 내성으로 판독하기를 권장하고 있으므로 아래의 경우처럼 감수성 결과를 보이는 cefepime의 결과를 내성으로 바꾸어 보고해야 함. 이 문제의 균은 ATCC700603으로 CTX-18 ESBL을 생산하는 균주로 2010년 판독기준에 따라 해석하면 ceftazidime, aztreonam, cettriaxone, cefotaxime 4가지 항균제 모두 I, R에 해당하며 cefepime의 경우 감수성인 MIC 결과를 보이나 내성으로 바꾸어 해석하여 보고한 것을 정답으로 인정. R 예시) 대한임상검사정도관리협회 임상미생물학분과 정도관리 2010년 1차
 대한임상검사정도관리협회 임상미생물학분과 정도관리 2010년 1차.")
33
1 항균제 선택보고시 오류분석과 해결방법 2 균종별, 항균제별 취약점 분석 3 자동화 기기를 이용시 오류분석과 해결방법

34
Automated test methodology based on the MIC technique
A mimiaturized and abbreviated version of the doubling dilution technique for MICs determined by the microdilution method. Reduce turnaround times Increase efficiency, and Improve cost-effectiveness Each AST card contains 64 microwells. A control well containing only microbiological culture medium is resident on all cards, with the remaining wells containing premeasured amounts of specific antimicrobials combined with culture medium. The organism suspension to be tested must be diluted to a standardized concentration in 0.45% saline before being used to rehydrate the antimicrobial medium within the card. The card is then filled, sealed, and placed into the instrument incubator/reader, either automatically of manually. The instrument monitors the growth of each well in the card over a defined period of time (upto 18 hours for bacteria or up to 36 hours for yeast) At the completion of the incubation cycle, MIC values are determined for each antimicrobial contained on the card. Each AST card contains selected antimicrobials in varying concentrations, dried with a microbiological culture medium.
 At the completion of the incubation cycle, MIC values are determined for each antimicrobial contained on the card. Each AST card contains selected antimicrobials in varying concentrations, dried with a microbiological culture medium.")
35
Antibiotic Susceptibility Test by Automated Instrument System
Repetitive mornitoring of bacterial growth Growth Pattern Parameters : area, magnitude, rate Standardization of the reading of end points

36
Advanced Expert System : automated review and verification
Programmed software : algorithms or rules Impossible or unusual phenotypes : flag Unlikely resistant patterns or rare antibiogram phenotypes Anti-biogram to predict resistant mechanism-modify test report ESBL이 검출된 환자로 advanced expert rule이 적용된 예

37
Expected MIC distribution for ESBL/AmpC/Acquired penicillinase
E. coli with an ESBL Expected MIC distribution for ESBL/AmpC/Acquired penicillinase Observed MIC ESBL이 검출된 환자로 advanced expert rule이 적용된 예 Correction proposed : Reported R

38
Major 3 automated systems MicroScan (Siemens) Vitek 2 (bioMerieux)
Phoenix System (Becton-Dickinson) Results by system used for testing (CAP survey 2011 Bacteriology) Staphylo-coccus spp., Agent: Oxacillin Test system No. of Labs Susceptible intermediate Resistant Agar Dilution Broth Macrodilution BD Phoenix E test Microdilution- In House MicroScan Sensititre Vitek Vitek 2 4 10 103 8 17 898 15 52 1085 9 84 7 875 25 1071 - 1 19 2 23 27 14
 Results by system used for testing (CAP survey 2011 Bacteriology) Staphylo-coccus spp., Agent: Oxacillin. Test system. No. of. Labs. Susceptible. intermediate. Resistant. Agar Dilution. Broth Macrodilution. BD Phoenix. E test. Microdilution- In House. MicroScan. Sensititre. Vitek. Vitek")
39
Acceptable Discrepancy Rates to assess AST,
Ideally, when evaluating a large collection of unselected clinical Isolates, very major discrepancy rates should be less than 1.5%, and major discrepancies should occur with less than 3% when calculated based on all isolates. VME (중대오류): Very major error – 표준법에서 내성이고 직접법에서 감수성 ME (대오류): Major error – 표준법에서 감수성이고 직접법에서 내성 mE (소오류): minor error 표준법과 직접법 둘 중 하나가 중간이고, 다른 하나가 내성 혹은 감수성인 경우 CLSI. Approved guideline M23-A
: Very major error – 표준법에서 내성이고 직접법에서 감수성. ME (대오류): Major error – 표준법에서 감수성이고 직접법에서 내성. mE (소오류): minor error 표준법과 직접법 둘 중 하나가 중간이고, 다른 하나가 내성 혹은 감수성인 경우. CLSI. Approved guideline M23-A")
40
자동화기기를 이용한 항생제 감수성 검사의 정확도
그람음성균에 대한 항균제감수성검사의 정확도는 Vitek 2, Phoenix는 균종-항균제 조합수로 계산할 때 99.2%, 99.0%의 높은 정확도를 보였다. J Clin Microbiol 2004;42:7-11 J Clin Microbiol 2004;42: 그람양성알균에 대해서 오류의 종류를 분석시, MicroScan의 경우 VME 1.1%, ME 1.1%, mE 3.12%이며, Phoenix의 경우 VME 1.1%, ME 0.8%, mE 1.7%로 나타났다. Korean J Lab Med 2009;29:25-34 VME (중대오류): Very major error – 표준법에서 내성이고 직접법에서 감수성 ME (대오류): Major error – 표준법에서 감수성이고 직접법에서 내성 mE (소오류): minor error 표준법과 직접법 둘 중 하나가 중간이고, 다른 하나가 내성 혹은 감수성인 경우
: Very major error – 표준법에서 내성이고 직접법에서 감수성. ME (대오류): Major error – 표준법에서 감수성이고 직접법에서 내성. mE (소오류): minor error 표준법과 직접법 둘 중 하나가 중간이고, 다른 하나가 내성 혹은 감수성인 경우.")
41
자동화기기를 이용한 항생제 감수성 검사의 정확도
Evaluation of the VITEK 2 system for susceptibility testing of Gram-negative Bacilli 1,067 organism-antibiotic combinations Overall agreement rate of 97.6% (By comparing the results using the broth microdilution method) Very major errors (0.2%) major errors (0.4%) Minor error : Reported as susceptible or resistant with VITEK2 system and intermediate by the reference test or intermediate with the VITEK2 system and susceptible or resistant by the reference test. Major error : Reported as resistant with the VITEK2 system and susceptible by the reference test Very major errors : reported as susceptible with the VITEK 2 and resistant by the reference test MB method : microdilution method according to the NCCLS guidelines as a reference J Clin Microbiol, Oct. 2003, p
 Very major errors (0.2%) major errors (0.4%) Minor error : Reported as susceptible or resistant with VITEK2 system and intermediate by the reference test or intermediate with the VITEK2 system and susceptible or resistant by the reference test. Major error : Reported as resistant with the VITEK2 system and susceptible by the reference test. Very major errors : reported as susceptible with the VITEK 2 and resistant by the reference test. MB method : microdilution method according to the. NCCLS guidelines as a reference. J Clin Microbiol, Oct. 2003, p")
42
자동화기기를 이용한 항생제 감수성검사시 고려할 점 I
Fastidious Bacteria : Hemophilus and other fasticious gram-negative bacteria will not grow in Mueller-Hinton broth that is not supplemented with growth enrichments. If there is inadequate growth in the growth well, the MIC results from the fastidious microorganisms are not valid. Alternative method should be used. If there is inadequate growth in the growth well, the MIC results from the fastidious microorganisms are not valid (the biochemical results are not valid), and an alternative method should be used.
, and an alternative method should be used.")
43
자동화기기를 이용한 항생제 감수성검사시 고려할 점 II
2. Effect of Inoculum size (접종량효과) : Elevated MICs with beta-lactam antimicrobials (e.g aztreonam) may be observed if panels are overinoculated with microorganisms such as Pseudomonas aeruginosa, Serratia spp., Proteus spp., Morganella spp., and Providencia spp. : Elevated MICs with fluoroquinolones, lincosamides and macrolides with Staphylococci when compared with the reference method. Inoculum should be prepared with Turbidity or Prompt methods.
 : Elevated MICs with beta-lactam antimicrobials (e.g aztreonam) may be observed if panels are overinoculated with microorganisms such as Pseudomonas aeruginosa, Serratia spp., Proteus spp., Morganella spp., and Providencia spp. : Elevated MICs with fluoroquinolones, lincosamides and macrolides with Staphylococci when compared with the reference method. Inoculum should be prepared with Turbidity or Prompt methods.")
44
자동화기기를 이용한 항생제 감수성검사시 고려할 점 II
Inoculum concentration is critical with these antimicrobials as their mechanism of action involves disruption of bacterial cell wall synthesis. Exercise care in preparing the accurate 0.5 McFarland suspension If an intermediate or resistant interpretation is obtained from these antimicrobic organism combinations, an alternative method of obtaining a susceptibility result should be used prior to reporting results. Inoculum should be prepared with Turbidity or Prompt methods.

45
S. pneumoniae Effect of Inoculum size
Incorrectly reported !! Antimicrobials # S I R % Acceptable Acceptable Response Cefepime 277 5 120 152 98.2 I, R Cefotaxime meningitis 243 9 23 211 86.8 Cefotaxime non-meningitis 832 81 251 500 90.3 Ceftriaxone meningitis 472 16 63 393 83.3 Ceftriaxone non-meningitis 1390 157 517 716 88.7 상기 S.pneumoniae는 multidrug resistant 균주였는데 일부 기관에서 cefepime, cefotaxime, cetriaxone 등의 항균제에 대해 감수성으로 잘못 보고하였다. The most likely reasons for the erroneous susceptible results include; 1) failure to follow the manufacturer’s recommendations (including QC) precisely if using a commercial test system; 2) failure to use the appropriate breakpoints as listed in CLSI for S. pneumoniae; amd 3) failure to pay strict sttention to inoculum preparation. S. Pneumoniae are fragile organisms which can readily lyse on agar plates or in liquid media. When preparing the inoculum suspension, care should be taken to: 1) use colonies no older than hours grown on a nonselective agar medium (e.g., BAP) and 2) prepare the inoculum suspension, standardize to a McFarland 0.5 standard and continue with the specific inoculation procedure for the test system without delay. Use of old colonies or allowing organisms to remain in liquid suspension for loger than 15 minutes could result in a significant decrease in numbers of viable organisms and false susceptible results. S. pneumoniae are fragile organisms which can readily lyse on agar plates or in liquid media. standardize to a McFarland 0.5 standard without delay use colonies no older than hours 예시) CAP survey Bacteriology 2010, D-B
 failure to follow the manufacturer’s recommendations (including QC) precisely if using a commercial test system; 2) failure to use the appropriate breakpoints as listed in CLSI for S. pneumoniae; amd 3) failure to pay strict sttention to inoculum preparation. S. Pneumoniae are fragile organisms which can readily lyse on agar plates or in liquid media. When preparing the inoculum suspension, care should be taken to: 1) use colonies no older than hours grown on a nonselective agar medium (e.g., BAP) and 2) prepare the inoculum suspension, standardize to a McFarland 0.5 standard and continue with the specific inoculation procedure for the test system without delay. Use of old colonies or allowing organisms to remain in liquid suspension for loger than 15 minutes could result in a significant decrease in numbers of viable organisms and false susceptible results. S. pneumoniae are fragile organisms which can readily lyse on agar plates or in. liquid media. standardize to a McFarland 0.5 standard without delay. use colonies no older than hours. 예시) CAP survey Bacteriology 2010, D-B.")
46
자동화기기를 이용한 항생제 감수성검사시 고려할 점
자동화기기를 이용한 항생제 감수성검사시 고려할 점 3. Mixed cultures : The main source of error in both bacterial identification and antimicrobial susceptibility testing is mixed cultures. If the colony morphology of the isolated organisms suggests a mixed infection or species other than indicated by the automated system, the purity of a positive culture was controlled several times: (i) by Gram staining (ii) by subculture and so on.
 by Gram staining. (ii) by subculture and so on.")
47
자동화기기를 이용한 항생제 감수성검사의 한계점 I
Vitek 2 system (bioMerieux) Gram Postive Susceptibility Card (AST-P600, AST-P601) : To determine the susceptibility of Staphylococcus spp. and Enterococcus spp. Perform an alternative method of testing prior to reporting of results for the following antibiotic/organism combination Erythromycin: Streptococcus agalactiae
 Gram Postive Susceptibility Card (AST-P600, AST-P601) : To determine the susceptibility of Staphylococcus spp. and. Enterococcus spp. Perform an alternative method of testing prior to reporting of results for the following antibiotic/organism combination. Erythromycin: Streptococcus agalactiae.")
48
자동화기기를 이용한 항생제 감수성검사의 한계점
자동화기기를 이용한 항생제 감수성검사의 한계점 The ability of the AST card to detect resistance with the following combination(s) is unknown because resistant strains were not available at time of comparative testing: Ampicillin: Streptococcus agalactiae Benzylpenicillin: Streptococcus agalactiae Linezolid: Enterococcus spp., Staphylococcus spp., Streptococcus agalactiae Tigecycline: Enterococcus spp., Staphylococcus spp., Streptococcus spp. Habekacin : Staphylococcus spp.
 is unknown because resistant strains were not available at time of comparative testing: Ampicillin: Streptococcus agalactiae. Benzylpenicillin: Streptococcus agalactiae. Linezolid: Enterococcus spp., Staphylococcus spp., Streptococcus agalactiae. Tigecycline: Enterococcus spp., Staphylococcus spp., Streptococcus spp. Habekacin : Staphylococcus spp.")
49
자동화기기를 이용한 항생제 감수성검사의 한계점
자동화기기를 이용한 항생제 감수성검사의 한계점 Vitek 2 system (bioMerieux) Gram Negative Susceptibility Card (AST-N131, AST-N224) : To determine the susceptibility of clinically significant aerobic Gram-negative bacilli Perform an alternative method of testing prior to reporting of results when an intermediate or resistant result is obtained with the following antibiotic/organism combination(s): Amoxicillin/Clavulanic Acid: Proteus spp.
 Gram Negative Susceptibility Card (AST-N131, AST-N224) : To determine the susceptibility of clinically significant aerobic Gram-negative bacilli. Perform an alternative method of testing prior to reporting of results when an intermediate or resistant result is obtained with the following antibiotic/organism combination(s): Amoxicillin/Clavulanic Acid: Proteus spp.")
50
자동화기기를 이용한 항생제 감수성검사의 한계점
자동화기기를 이용한 항생제 감수성검사의 한계점 Perform an alternative method of testing prior to reporting of results for the following antibiotic/organism combination(s): Amikacin: Acinetobacter baumannii Amoxicillin/Clavulanic acid: Providencia spp. Ampicillin: Citrobacter spp., Enterobacter spp., Pantoea spp., Serratia spp. Aztreonam: Pseudomonas spp. Imipenem : Morganella morganii, Proteus spp., Providencia spp. Meropenem : Acinetobacter spp.
: Amikacin: Acinetobacter baumannii. Amoxicillin/Clavulanic acid: Providencia spp. Ampicillin: Citrobacter spp., Enterobacter spp., Pantoea spp., Serratia spp. Aztreonam: Pseudomonas spp. Imipenem : Morganella morganii, Proteus spp., Providencia spp. Meropenem : Acinetobacter spp.")
51
Imipenem : Proteus spp. 획득성 내성이 없는 균종으로 모든 β-lactam계에 감수성인 균주였으나,
기관중 17기관에서 위내성률을 보임. 정도관리에 사용한 균종은 획득성 내성이 없는 균종으로 모든 β-lactam에 감수성이었는데도 불구하고, MIC법으로 imipenem 감수성검사를 실시한 44곳 중 imipenem에 I, R로 보고한 기관이 17곳(38.6%)으로 유일하게 심한 위내성율을 보였습니다. 이는 모두 VITEK2를 사용하는 기관으로 특정 panel 또는 lot에 문제가 있었을 것으로 추정됩니다. 특히 imipenem은 열에 취약하여 불활화됨으로써 imipenem 내성 균종의 가성유행(pseudooutbreak)가 종종 보고되는 항균제임으로 이번에 imipenem 감수성결과를 위내성으로 보고한 기관은 imipenem 감수성검사에 대한 정도관리에 더 주의하시기 바랍니다.
으로 유일하게 심한 위내성율을 보였습니다. 이는 모두 VITEK2를 사용하는 기관으로 특정 panel 또는 lot에 문제가 있었을 것으로 추정됩니다. 특히 imipenem은 열에 취약하여 불활화됨으로써 imipenem 내성 균종의 가성유행(pseudooutbreak)가 종종 보고되는 항균제임으로 이번에 imipenem 감수성결과를 위내성으로 보고한 기관은 imipenem 감수성검사에 대한 정도관리에 더 주의하시기 바랍니다.")
52
자동화기기를 이용한 항생제 감수성검사의 한계점
자동화기기를 이용한 항생제 감수성검사의 한계점 The ability of the AST card to detect resistance with the following combination(s) is unknown because resistant strains were not available at the time of comparative testing: Ertapenem: E. coli, K. pneumoniae, C. freundii, C. koseri, E. aerogenes, E. cloacae, K. oxytoca (excluding ESBL producing strains), M. morganii, P. mirabilis, P. vulgaris, S. marcescens Tigecycline: C. freundii, E. cloacae, E. coli, K. oxytoca, K. pneumoniae, C. koseri, E. aerogenes, S. marcescens
 is unknown because resistant strains were not available at the time of comparative testing: Ertapenem: E. coli, K. pneumoniae, C. freundii, C. koseri, E. aerogenes, E. cloacae, K. oxytoca (excluding ESBL producing strains), M. morganii, P. mirabilis, P. vulgaris, S. marcescens. Tigecycline: C. freundii, E. cloacae, E. coli, K. oxytoca, K. pneumoniae, C. koseri, E. aerogenes, S. marcescens.")
53
자동화기기를 이용한 항생제 감수성검사의 한계점 III
MicroScan system (Siemens) Dried Overnight Gram Negative Panels To detect Nalidixic acid resistance in Salmonella strains is unknown because resistant strains were not available at the time of comparative testing. An alternative method should be used. 2010 SIEMENS user meeting 자료에서 발췌. 2010년 자료이지만 당시 한계점이 아직 개선되지 못했고, 이후 추가된 문제점이 없음을 확인.
 Dried Overnight Gram Negative Panels. To detect Nalidixic acid resistance in Salmonella strains is unknown because resistant strains were not available at the time of comparative testing. An alternative method should be used SIEMENS user meeting 자료에서 발췌. 2010년 자료이지만 당시 한계점이 아직 개선되지 못했고, 이후 추가된 문제점이 없음을 확인.")
54
자동화기기를 이용한 항생제 감수성검사의 한계점
자동화기기를 이용한 항생제 감수성검사의 한계점 Dried Overnight Gram Positve Panels To detect resistance of Meropenem among Listeria monocytogenes, and Trovafloxacin among β-hemolytic streptococcus, is unknown because resistant strains were not available at the time of comparative testing.