Download presentation
1
경희의료원 심장내과 R1 박소영 / Prof 김진배
MGR Case 1 경희의료원 심장내과 R1 박소영 / Prof 김진배

2
Dyspnea, NYHA Ⅳ (onset: 1 day ago) P/I>
C/C> Dyspnea, NYHA Ⅳ (onset: 1 day ago) P/I> F/74, CHF, A fib, HTN & Lt renal infart s/p Lt renal artery thrombectomy 과거력 있는 자로 내원 1일 전부터 resting dyspnea 발생하여 ER 통해 admission.
 P/I> F/74, CHF, A fib, HTN & Lt renal infart s/p Lt renal artery thrombectomy 과거력 있는 자로 내원 1일 전부터 resting dyspnea 발생하여 ER 통해 admission.")
3
Past history> DM/HTN/Tb/Hepatitis (-/+/-/-)
’11 Lt renal infarction s/p Lt renal a thrombectomy CHF, DCMP, A fib Drug history> β-blocker (carvedilol, dilatrend) 3.125mg qd/6.25mg qd Warfarin 3mg qd, Clopidogrel 75mg qd Loop diuretics (Fusosemide, Lasix) 40mg qd Personal history> Alcohol(-) smoking(-)
 3.125mg qd/6.25mg qd. Warfarin 3mg qd, Clopidogrel 75mg qd. Loop diuretics (Fusosemide, Lasix) 40mg qd. Personal history> Alcohol(-) smoking(-)")
4
Initial lab finding CBC/DC Chemistry Urinalysis
14,920/mm² g/dl – 38.2 % - 332K, (Seg. 75.6%) PT (INR) sec (1.70) aPTT sec Chemistry Prot/Alb 6.9/4.2 g/dL TB/DB /0.31 mg/dL AST/ALT 19/18 IU/L ALP/γGT /39 IU/L BUN/Cr 10/0.6 mg/dL Na/K/Cl /3.6/101 mEq/L Ca/P/Mg 8.7/3.1/2.1 mg/dL CK/CK-MB/TnI /1.2/0.02 U/L CRP mg/dL pro BNP pg/mL Urinalysis RBC 0~1/HPF WBC 0~1/HPF
 PT (INR) 19.7 sec (1.70) aPTT 36.4 sec. Chemistry. Prot/Alb 6.9/4.2 g/dL TB/DB 1.83/0.31 mg/dL. AST/ALT 19/18 IU/L ALP/γGT 74/39 IU/L. BUN/Cr 10/0.6 mg/dL Na/K/Cl 141/3.6/101 mEq/L. Ca/P/Mg 8.7/3.1/2.1 mg/dL CK/CK-MB/TnI 37/1.2/0.02 U/L. CRP 1.60 mg/dL pro BNP 4461 pg/mL. Urinalysis. RBC 0~1/HPF WBC 0~1/HPF.")
5
Review of System General generalized weakness (-)
fever (-) chill (-) fatigue (-) edema (-) sweating (+) Skin rash (-) pigmentation (-) itching (-) Head/ENT headache (-) sore throat (-) Respiratory cough (-) sputum (-) dyspnea (+) hemoptysis (-) Cardiovascular chest pain (-) palpitation (-) exertional dyspnea (+) orthopnea (+) nocturnal dyspnea (+) syncope (-)
 chill (-) fatigue (-) edema (-) sweating (+) Skin rash (-) pigmentation (-) itching (-) Head/ENT headache (-) sore throat (-) Respiratory cough (-) sputum (-) dyspnea (+) hemoptysis (-) Cardiovascular chest pain (-) palpitation (-) exertional dyspnea (+) orthopnea (+) nocturnal dyspnea (+) syncope (-)")
6
Review of System GI anorexia/nausea/vomiting/diarrhea/constipation(-/-/-/-/-) abdominal pain (-) epigastric discomfort (-) abdominal distension (-) Urogenital flank pain (-) dysuria (-) urgency (-) frequency (-) retension (-) pyuria (-) Musculoskeletal pain (-) pph. edema (-) weakness (-) arthralgia (-) Nerve system fainting (-) dizziness (-) sensory loss (-) motor weakness (-) tremor (-)
 abdominal pain (-) epigastric discomfort (-) abdominal distension (-) Urogenital flank pain (-) dysuria (-) urgency (-) frequency (-) retension (-) pyuria (-) Musculoskeletal pain (-) pph. edema (-) weakness (-) arthralgia (-) Nerve system fainting (-) dizziness (-) sensory loss (-) motor weakness (-) tremor (-)")
7
Physical examination Initial V/S 120/70 mmHg- 72회/분- 22회/분 -36.0°C
General Alert consciousness Chronic ill looking appearance Head/ENT Isocoric pupil c pupil light reflex (++/++) Neck vein engorgement (-/-) Neck lymph node enlargement (-/-) Chest Symmetric chest expansion Regular heart beat without murmur Clear breathing sound without rale or wheezing
 Neck vein engorgement (-/-) Neck lymph node enlargement (-/-) Chest Symmetric chest expansion. Regular heart beat without murmur. Clear breathing sound without rale or wheezing.")
8
Physical examination V 100 Abdomen Soft and obese abdomen
No shifting dullness Normoactive bowel sound Abdominal tenderness/rebound tenderness (-/-) Back/Ext Costovertebral angle tenderness (-/-) Pretibial pitting edema (-/-) Motor/Sensory V 100
 Back/Ext Costovertebral angle tenderness (-/-) Pretibial pitting edema (-/-) Motor/Sensory. V")
9
Initial chest X-ray

10
Initial EKG (11:46 at ER) HR 80bpm QT/QTc 470/538 :46
 HR 80bpm QT/QTc 470/ :46")
11
Initial assessment>
CHF acute exacerbation Paroxysmal atrial fibrillation DCMP HTN Diuretics (Furosemide) IV Beta-blocker (Carvedilol) 6.25mg PO ACE inhibitor (Perindopril) 2mg PO Vasodilator (Nitrate) IV
 IV. Beta-blocker (Carvedilol) 6.25mg PO. ACE inhibitor (Perindopril) 2mg PO. Vasodilator (Nitrate) IV.")
13
F/U Electrolyte Na / K / Cl 141 / 3.6 / 101 → 139 / 2.9 / 100
Ca / P / Mg / 3.1 / 2.1 → 8.1 / 2.7 / 2.1

14
Telemetry monitoring

15
Telemetry monitoring

16
F/U EKG (20:42) :42
 :42")
17
F/U EKG (20:42)
")
18
F/U EKG (21:14)
")
19
F/U EKG (23:17) after isoproterenol
 after isoproterenol")
20
F/U EKG (퇴원당시)
")
21
Discharge medication Β-blocker (Carvedilol, Dilatrend) 3.125mg bid
ACE inhibitor (Perindopril, Acertil) 4mg qd Digoxin 1.125mg qd Aldosterone antagonist (Spironolactone, Aldacton) 25mg qd Loop diuretics (Furosemide, Lasix) 40mg qd Clopidogrel (Krivix) 75mg Warfarin 3mg qd
 4mg qd. Digoxin 1.125mg qd. Aldosterone antagonist (Spironolactone, Aldacton) 25mg qd. Loop diuretics (Furosemide, Lasix) 40mg qd. Clopidogrel (Krivix) 75mg. Warfarin 3mg qd.")
22
Case 2

23
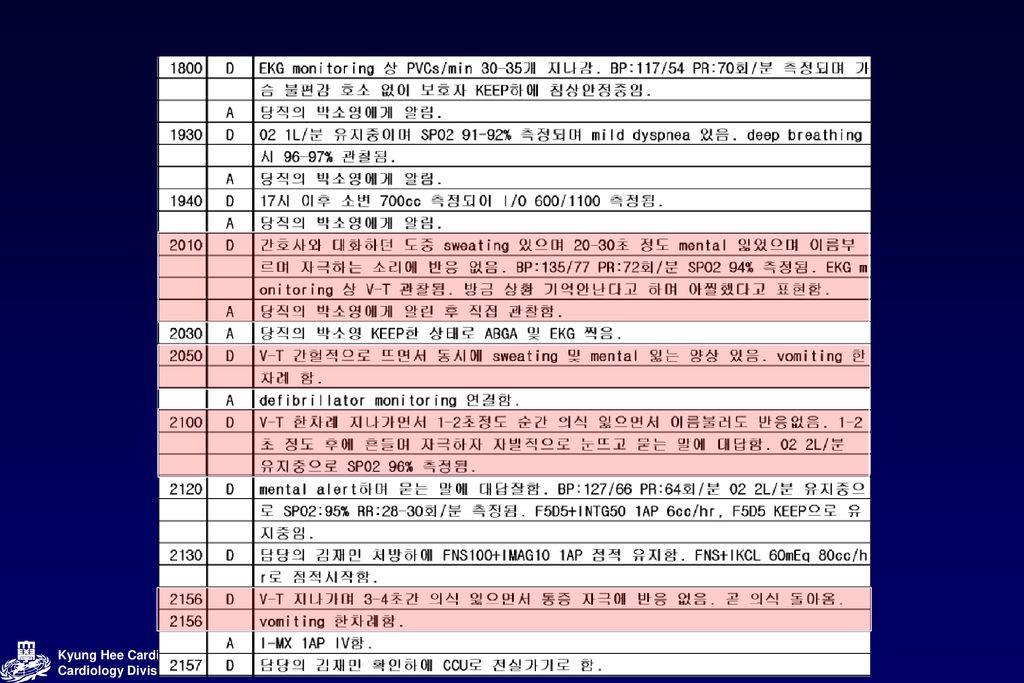
C/C> 발작을 했어요 o/s) 30 minutes ago P/I> F/82, Old Cb inf. HTN, A.fib, bradycardia, hypothyroidism & dementia medication중인 자, 최근 bradycardia로 pacemaker insertion 권유받았으나 refuse하였던 환자로 내원 당일 아침 10초 정도 의식 저하 있으면서 몸을 굽히며 비트는 양상의 발작 동반되고 수차례 반복되어 응급실 내원, 신경과 진료위해 대기 중 EKG monitoring에서 VT 소견과 함께 발작 및 의식 저하있어 내과 진료 의뢰됨. Old Cb inf. HTN, A.fib, bradycardia, hypothyroidism으로 본원 IC, IE f/u중이며 local에서 dementia medication중인 82세 여환, 최근 Bradycardia로 김진배교수님 외래에서 Pacemaker insertion필요성 및 급사가능성 설명받았으나 증상없어서 refuse하고 po medication처방받았던 환자로 내원당일 아침에 갑자기 경련하는 듯한 모습과 함께 쓰러졌고 이후 의식되찾았으나 계속 의식저하와 함께 경련하는 모습 반복(약 10초~30분가량)되어 응급실내원함. 응급실내원 후 monitoring상 ECG에 VT 지나가면서 경련 및 의식저하소견있어 내과진료의뢰됨.
 30 minutes ago P/I> F/82, Old Cb inf. HTN, A.fib, bradycardia, hypothyroidism & dementia medication중인 자, 최근 bradycardia로 pacemaker insertion 권유받았으나 refuse하였던 환자로 내원 당일 아침 10초 정도 의식 저하 있으면서 몸을 굽히며 비트는 양상의 발작 동반되고 수차례 반복되어 응급실 내원, 신경과 진료위해 대기 중 EKG monitoring에서 VT 소견과 함께 발작 및 의식 저하있어 내과 진료 의뢰됨. Old Cb inf. HTN, A.fib, bradycardia, hypothyroidism으로 본원 IC, IE f/u중이며 local에서 dementia medication중인 82세 여환, 최근 Bradycardia로 김진배교수님 외래에서 Pacemaker insertion필요성 및 급사가능성 설명받았으나 증상없어서 refuse하고 po medication처방받았던 환자로 내원당일 아침에 갑자기 경련하는 듯한 모습과 함께 쓰러졌고 이후 의식되찾았으나 계속 의식저하와 함께 경련하는 모습 반복(약 10초~30분가량)되어 응급실내원함. 응급실내원 후 monitoring상 ECG에 VT 지나가면서 경련 및 의식저하소견있어 내과진료의뢰됨.")
24
Past Medical History Medication Personal History
HTN /DM /Tbc /Hepatitis (+/-/-/-) A fib, hypothyroidism, Old CVA inf, dementia Medication ARB (Fimasartan, Kanarb) 60mg qd Statin (Pravastatin, Mevalotin) 20mg qd Warfarin 2.5mg qd Levothyroxine 75mcg qd Personal History Alcohol (-), smoking (+): 30 py
 A fib, hypothyroidism, Old CVA inf, dementia. Medication. ARB (Fimasartan, Kanarb) 60mg qd. Statin (Pravastatin, Mevalotin) 20mg qd. Warfarin 2.5mg qd. Levothyroxine 75mcg qd. Personal History. Alcohol (-), smoking (+): 30 py.")
25
Review of System Uncheckable status

26
Physical examination V/S General drowsy consciousness Head and Neck
210/120mmHg – 49회/min- 20회/min- 36.0°C General drowsy consciousness chronically-ill looking appearance Head and Neck Isocoric pupil c pupil light reflex (++/++) Thorax symmetric chest expansion clear breathing sound without rale Regular heart beat without murmur PMI at 5th ICS x MCL 170/ %
 Thorax. symmetric chest expansion. clear breathing sound without rale. Regular heart beat without murmur. PMI at 5th ICS x MCL. 170/ %")
27
Initial Lab Findings CBC/DC Chemistry U/A
9170/mm² g/dl – 33.9 %- 240K(seg : 81%) aPTT sec PT(INR) (1.72) Chemistry AST/ALT /19U/L BUN/Cr 16/0.8mg/dL TB/DB /0.17 mg/dL Na/K/Cl /3.6/106mmol/L ALP/GGT /44 U/L Ca/P/Mg / 3.1 /1.8 mg/dL Protein/Alb /3.3 g/dL CRP mg/dL CK/CK-MB UL /2.8 ng/mL TnI ng/mL U/A RBC 0~1/HPF WBC 0-1/HPF
 aPTT 34.8 sec PT(INR) 19.9 (1.72) Chemistry. AST/ALT 33/19U/L BUN/Cr 16/0.8mg/dL. TB/DB 0.60/0.17 mg/dL Na/K/Cl 139/3.6/106mmol/L. ALP/GGT 95/44 U/L Ca/P/Mg 8.0/ 3.1 /1.8 mg/dL. Protein/Alb 6.1/3.3 g/dL CRP 1.29mg/dL. CK/CK-MB 135 UL /2.8 ng/mL TnI 0.15 ng/mL. U/A. RBC 0~1/HPF WBC 0-1/HPF.")
28
Initial chest X-ray .

29
Initial EKG 정상 axis 이며 HR 30회의 bradycardia 관찰되고 있으며 RR interval regular 하고 P wave 관찰 되지 않는 Af c junctional eacpae bradycardia 로 판단됩니다.

30
EKG ( :09) HR 45 회정도의 bradycardia 관찰되고 있으며 정상 axis 보이고 있습니다 RR interval regular 하나 p wave 보이지 않는 junction rhythm 보이고 있으며 QT prologation 관찰 되고 있습니다. V2 ~ 3 까지 T wave inversion 보이고 있습니다.

31
EKG ( :09) 이어 찍은 EKG 에서 T wave 바로 VPC 나오기 시작하면서 baseline 흔들리는 양상 관찰 되고 있습니다.
 이어 찍은 EKG 에서 T wave 바로 VPC 나오기 시작하면서 baseline 흔들리는 양상 관찰 되고 있습니다.")
32
EKG ( :13 – DC shock 1st) VPC 반복적으로 나오면서 Torsades de pointes 관찰되고 있었으며 ER에서 DC cardioversion 시행하였습니다.
 VPC 반복적으로 나오면서 Torsades de pointes 관찰되고 있었으며 ER에서 DC cardioversion 시행하였습니다.")
33
EKG ( :14 – DC shock 2nd)
")
34
EKG (12-02-04 11:30~ after isoproterenol)
")
35
EKG ( :48)
")
36
Temporary pacemaker Insertion

37
EKG ( :22)
")
38
EKG ( :03)
")
39
Permanent pacemaker Insertion

40
EKG ( :24)
")
41
CXR ( )
")
42
EKG ( :24)
")
43
Clinical Course Permanent Pacemaker insertion Temporary Pacemaker
2/510:58 11:13 11:14 11:25 12:00 19:00 2/714:00 Temporary Pacemaker insertion Isoproterenol 4㎍/min D.C cardioversion 200J 11:13 DC shock 200J 11:14 DC shock 200J + atopine IV 11:22 Mag 1! IV 11:25 isoprotererol 60ml/hr 12:00 isoprotererol 80ml/hr Isoproterenol 5㎍/min D.C cardioversion 200J Atropine 0.5mg IVSS



 Case 1.>")




2006.04.27 C.C ) for DM manage P.I ) DM 으로 18 년전 부터 외래 F/U 하며 DM 조절 중 인 환자로 poor oral intake 있어 약 한달.>")

 3 days ago CC: Feveronset) 3 days ago PI : F/29, 5 년전 첫아기 임신 8 개월째에.>")







 C.C. > Anorexia o/s) 내원 약 4 주전 P. I. > 1 년 간 7kg 의 weight loss 있었고, 두 달 전 시행한 abd CT 및 위내시경에서 양성종양 발견되어 observation 하던 중, 최 근 한 달.>")
 Adm 2012.03.28 주소 Cough onset time) 내원 1 달 전 현병력 60 세 여자환자. HTN, dyslipidemia 로 타 병원에서 medication.>")

