Download presentation
Presentation is loading. Please wait.

1
ROLE OF NEPHROLOGIST IN POISONING
2
Poisoining - Role of Nephrologist
Iatrogenic drug toxicity AKI due to poisons Metabolic consequence –requiring intervention Removal by altering Urine p H Drug removal by extracorporeal techniques hemodialysis hemoperfusion

3
Epidemiology in developed world
1 % of all admissions 10 – 15% of ICU admissions Age :25 yrs F > M Accidental - more common in children 1-2 % mortality Declining trend in mortality because of general prevalence of safer drugs

4
Major public health concern
AAPCC : Reported million Urine alkalinization 8654 Hemodialysis Hemoperfusion 29 Death <6 years 116 6 -19 years 153 >19 years 805 Watson WA, Am J Emerg Med 2005:13:

5
Pattern of drug use with suicidal intent
Paracetamol 29 Benzodiazepines 13 Antidepressants 11 Compound analgesics 10 NSAIDS 6 Aspirin 6 Street drugs 5 blockers 2 Antibiotics 2 Anticonvulsants 2 Household compounds 1 Theophylline 0.7 Lithium 0.7 Iron 0.5 Hypoglycemics 0.5 Others

6
Pattern of drug use with suicidal intent
Paracetamol 29 Benzodiazepines 13 Antidepressants 11 Compound analgesics 10 NSAIDS 6 Aspirin 6 Street drugs 5 blockers 2 Antibiotics 2 Anticonvulsants 2 Household compounds 1 Theophylline 0.7 Lithium 0.7 Iron 0.5 Hypoglycemics 0.5 Others

7
In developing world… Poisoning with animal & plant products
Hydrocarbons Agrochemicals

8
Diagnosis may not be straight forward…
Unexplained coma Unexplained ARF Unexplained metabolic disorder High anion gap metabolic acidosis Ethylene glycol Methanol Mixed acid base disorder Salicylates

9
Treatment -General Principles
Primary aim: ‘not to retrieve poison but to save life!’ Mainstay of treatment is supportive Spontaneous excretion / metabolism occurs Fluid balance Electrolyte abnormalities Acid base derangements Cardiovascular respiratory support

10
Direct nephrotoxicity
AKI in Poisoning Circulatory collapse Rhabdomyolysis Hepatorenal Syndrome Direct nephrotoxicity

11
Specific Nephrotoxicity
Heavy metals, Acetaminophen, Salicylates, Herbicides Specific Nephrotoxicity Amphetamines, Barbituarates,cocaine, Heroin,Methadone CO,snake venom , Arthropod, & Insect venoms ATN Myoglobinuric Hemoglobinuric ATN Crystalluric ATN CuSO4,venoms Ethylene glycol

12
SPECIFIC ANTIDOTES Benzodiazepine Flumazenil CO Oxygen
Cyanide Amyl nitrate,Sodium nitrite,thiosulfate, Edetate dicobalt Digoxin Antibodies Ethylene glycol Ethanol Iron salts Desferoxamine Methanol Ethanol/ fomepizole Opiods Naloxone OPC atropine,P2AM Acetaminophen Methionine, N acetylcysteine

13
Prevention of drug absorption
Gastric lavage Activated charcoal

14
Drug removal by Diuresis
Diuresis at controlled pH 1. Salicylate (weak acid), excretion enhanced in alkaline urine (pH 8) 2. Amphetamine (weak alkali), excretion enhanced in acid urine(pH 5)
, excretion enhanced in alkaline urine (pH 8) 2. Amphetamine (weak alkali), excretion enhanced in acid urine(pH 5)")
15
Drugs amenable to FAD Phenobarbital Barbital Salicylate Chlorpropamide
Copper sulphate

16
Forced Alkaline Diuresis
GOAL : Alkalinise the urine and maintain a urine volume of > 6 ml/min (> 300 ml./hr) Fluids used : A - NS ml. B - 5% D. 400 ml +100 ml NaHCO3 C - NS ml ml KCl Contraindications: (a) Pulm. Oedema (b) Sr. Creat. > 300 mol/L
 Fluids used : A - NS 500 ml. B - 5% D. 400 ml +100 ml NaHCO3. C - NS ml ml KCl. Contraindications: (a) Pulm. Oedema. (b) Sr. Creat. > 300 mol/L.")
17
F A D 1st hour 500 ml. of ( A) is given Output < 350 ml/hr.
at the end of 1st hour. Output > 350 ml/hr Lasix 40 mg IV & continue 500 ml. of (B) for 1 hour Continue FAD Inflow volume = hrly output + 50 – 60 ml./hr (approx. 1.2 – 1.5 L/d positive balance) Output < 350ml./hr at the end of 2nd hour 2nd dose of Lasix 40 mg. and no fluids for the 3rd hour Alternate with solution (B)), (C) & (A) for 1 hour each (Discard excess solution if any and go to next type of solution). Output < 350 ml./hr at the end of 3rd hour STOP FAD
 for 1 hour. Continue FAD. Inflow volume = hrly output + 50 – 60 ml./hr. (approx. 1.2 – 1.5 L/d positive balance) Output < 350ml./hr at. the end of 2nd hour. 2nd dose of Lasix 40 mg. and no fluids for the 3rd hour. Alternate with solution (B)), (C) & (A) for 1 hour each. (Discard excess solution if any and. go to next type of solution). Output < 350 ml./hr at the. end of 3rd hour. STOP FAD.")
18
Forced Acid Diuresis 5% GNS (1 litre) over 2 hrs
Arginine 10 g i.v. over 30 min 5% GNS 500 ml every 2 hrs NH4 Cl 4g / 2hrs Maintain & monitor urine pH / S.K

19
Extra Corporeal Treatment- Indications
Progressive deterioration despite Intensive supportive treatment Midbrain suppression – hypothermia, hypotension Complications of coma – pneumonia , septicemia Impaired normal excretory function in the presence of hepatic / cardiac/ renal insufficiency

20
Extra Corporeal Treatment- Indications
Intoxication with agents with harmful metabolic / delayed effects e.g. methanol, ethylene glycol & paraquat Intoxicants whose removal are faster in dialysis or hemoperfusion than their natural route of elimination (liver / kidney) Critical blood level
 Critical blood level.")
21
Techniques- Hemodialysis
Small molecule removal by diffusion along a concentration gradient Size: Da (high flux-10000Da) Ineffective if lipid soluble or protein bound Routine indications as applicable in ARF PD inefficient
 Ineffective if lipid soluble or protein bound. Routine indications as applicable in ARF. PD inefficient.")
22
Hollow Fiber Dialyzers
Notes _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ __________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ __________________ _________________________________________________________ _________________________________________________________ ____________ Blood inlet header of a hollow fiber dialyzer Range of Dialyzers 22

23
Dialysate/Ultrafitrate
Solute Clearance Blood Membrane Dialysate/Ultrafitrate

24
Diffusive Solute Clearance
Blood Membrane Dialysate/Ultrafitrate

25
Diffusive Solute Clearance
Blood Membrane Dialysate/Ultrafitrate

26
HEMODIALYSIS – CIRCUIT

27
HEMODIALYSIS CIRCUIT

28
DIALYSIS MACHINE Adjustable inflow resistance dialysate blood
Negative pressure Dialysate pump

29
State of the Art: High Tech Equipment
Notes _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ __________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ __________________ _________________________________________________________ _________________________________________________________ ____________ 29

30
Techniques-Hemofiltration
Convective transport Size upto Da No advantage over HD except for aminoglycoside , desferroxamine

31
Convection 의미있는 중분자량의 제거를 위해서는 convective transport량이 50mL/min이 넘어야 한다.(이는 high-flux HD로는 불가능) Diffusive therapy : diffusion은 분자량에 의한 제한은 받으나 물질이동의 기본원리이다. Diffusion에 의한 driving force는 blood와 dialysate의 농도차이다. 즉, 분자량이 작을수록, 농도차가 클수록 diffusion은 더 빠르게 일어난다. diffusion의 저해요인은 membrane thickness이다. concentration gradient는 contercurrent flow와 high-flow rate으로 유지된다. Convective therapy : 사구체에서 blood로부터 solute를 제거할 때 쓰여지는 Mechanism이다. convection에서는 solute가 압력차이에 의해 발생하는 fluid flow에 의해 이동한다. 이상적인 convective membrane은 사구체와 같은 체효과를 갖는 것으로 albumin이하의 물질이 통과가능한 membrane이다. HF : 소분자량의 물질에 대한 청소율은 일정정도는 가능하나 diffusion에 의한 제거 만큼은 아니다. HD : 기존의 HD로는 convective transport는 제한을 받는다. (why:UF의 제한, tight membrane) high-flux HD : back-filtration고려해야 한다. tight membrane : not allow for the sieving of large solutes. Combining diffusion and convection : uremic toxin의 특성에 대한 지식부족을 감안할때 Small solute와 large solute둘다를 제거하는데는 diffusion과 convection에 의한 HDF라면, 전분자량에 걸친 가장 높은 청소율을 제공해 줄 수 있다. HDF는 동일상황에서 HD보다 10-15%의 높은 urea 청소율을 제공해준다. 31
 high-flux HD : back-filtration고려해야 한다. tight membrane : not allow for the sieving of large solutes. Combining diffusion and convection : uremic toxin의 특성에 대한 지식부족을 감안할때. Small solute와 large solute둘다를 제거하는데는 diffusion과 convection에 의한 HDF라면, 전분자량에 걸친 가장 높은 청소율을 제공해 줄 수 있다. HDF는 동일상황에서 HD보다 10-15%의 높은 urea 청소율을 제공해준다. 31.")
32
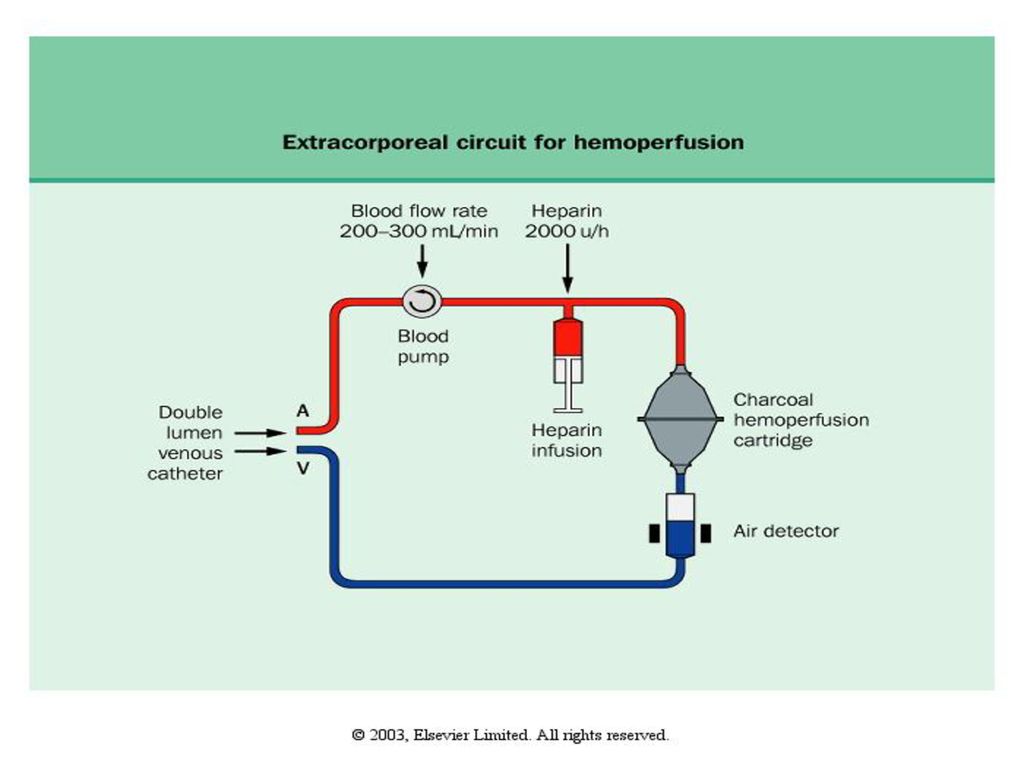
Techniques-Hemoperfusion
Direct contact with a adsorbent cartridge (charcoal, Amberlite) Thrombocytopenia Leucopenia Low fibrinogen Hypothermia Hypocalcemioa Hypoglycemia Time limited 4-8 hours
 Thrombocytopenia. Leucopenia. Low fibrinogen. Hypothermia. Hypocalcemioa. Hypoglycemia. Time limited 4-8 hours.")
33
Adsorption ADSORPTION: molecular adherence to the surface
의미있는 중분자량의 제거를 위해서는 convective transport량이 50mL/min이 넘어야 한다.(이는 high-flux HD로는 불가능) Diffusive therapy : diffusion은 분자량에 의한 제한은 받으나 물질이동의 기본원리이다. Diffusion에 의한 driving force는 blood와 dialysate의 농도차이다. 즉, 분자량이 작을수록, 농도차가 클수록 diffusion은 더 빠르게 일어난다. diffusion의 저해요인은 membrane thickness이다. concentration gradient는 contercurrent flow와 high-flow rate으로 유지된다. Convective therapy : 사구체에서 blood로부터 solute를 제거할 때 쓰여지는 Mechanism이다. convection에서는 solute가 압력차이에 의해 발생하는 fluid flow에 의해 이동한다. 이상적인 convective membrane은 사구체와 같은 체효과를 갖는 것으로 albumin이하의 물질이 통과가능한 membrane이다. HF : 소분자량의 물질에 대한 청소율은 일정정도는 가능하나 diffusion에 의한 제거 만큼은 아니다. HD : 기존의 HD로는 convective transport는 제한을 받는다. (why:UF의 제한, tight membrane) high-flux HD : back-filtration고려해야 한다. tight membrane : not allow for the sieving of large solutes. Combining diffusion and convection : uremic toxin의 특성에 대한 지식부족을 감안할때 Small solute와 large solute둘다를 제거하는데는 diffusion과 convection에 의한 HDF라면, 전분자량에 걸친 가장 높은 청소율을 제공해 줄 수 있다. HDF는 동일상황에서 HD보다 10-15%의 높은 urea 청소율을 제공해준다. ADSORPTION: molecular adherence to the surface or interior of the membrane 33
 Diffusive therapy : diffusion은 분자량에 의한 제한은 받으나 물질이동의 기본원리이다. Diffusion에 의한 driving force는 blood와 dialysate의 농도차이다. 즉, 분자량이 작을수록, 농도차가 클수록 diffusion은 더 빠르게 일어난다. diffusion의 저해요인은 membrane thickness이다. concentration gradient는 contercurrent flow와 high-flow rate으로 유지된다. Convective therapy : 사구체에서 blood로부터 solute를 제거할 때 쓰여지는 Mechanism이다. convection에서는 solute가 압력차이에 의해 발생하는 fluid flow에 의해 이동한다. 이상적인 convective membrane은 사구체와 같은 체효과를 갖는 것으로. albumin이하의 물질이 통과가능한 membrane이다. HF : 소분자량의 물질에 대한 청소율은 일정정도는 가능하나 diffusion에 의한 제거 만큼은 아니다. HD : 기존의 HD로는 convective transport는 제한을 받는다. (why:UF의 제한, tight membrane) high-flux HD : back-filtration고려해야 한다. tight membrane : not allow for the sieving of large solutes. Combining diffusion and convection : uremic toxin의 특성에 대한 지식부족을 감안할때. Small solute와 large solute둘다를 제거하는데는 diffusion과 convection에 의한 HDF라면, 전분자량에 걸친 가장 높은 청소율을 제공해 줄 수 있다. HDF는 동일상황에서 HD보다 10-15%의 높은 urea 청소율을 제공해준다. ADSORPTION: molecular adherence to the surface. or interior of the membrane. 33.")
34
CHARCOAL HEMOFILTER

36
Techniques-Hemodialysis & Hemoperfusion
Adsorption & diffusion →I choice Total removal in 4 hrs If Vd is small hrs if larger Vd e.g. Theophylline Amanita

37
Techniques-Exchange Transfusion
Hemolysis e.g. sodium chlorate , arsine Methemoglobinemia & sulfhemoglobinemia e.g. H2S

38
Drug level Hemodialysis Ethanol Methanol Ethylene glycol Lithium
Salicylate >5g/L >50 mg/ L >500mg/ l >4m.mol/L 2.5 m.mol/l if severe >800mg/L

39
Hemoperfusion Drug level Amanita Barbituarates Carbamazepine Paraquat
Theophylline Valproic acid Clinical severity >150 mg/ L Acute > 100mg/l Chronic > 40 mg/l >1g/l

40
Stabilize (airway , BP, Temp)
Identify drug or chemical antidotes Poisoned patient Oral ingestion Inhaled poison Dermal exposure Remove from environment Decontaminate Gastric lavage (< 1hr) Multiple dose activated charcoal Not improved Improved Improved Continue antidotes Altering Urine pH Hemodialysis Hemoperfusion Plasmapharesis, exchange blood transfusion Drug specific antibodies
 Multiple dose activated charcoal. Not improved. Improved. Improved. Continue antidotes. Altering Urine pH. Hemodialysis. Hemoperfusion. Plasmapharesis, exchange blood transfusion. Drug specific antibodies.")
41
POISOINING - GGH/MMC N = 951 Period 1997- 2003
snake bite (81), copper sulphate(44) Ethylene glycol poisoning 5 (4 required dialysis) Methanol 9 cases in the last year
, copper sulphate(44) Ethylene glycol poisoning 5 (4 required dialysis) Methanol 9 cases in the last year.")
42
POISOINING - GGH/MMC Annual conference of nephrology2002
ARF due to poisons over a 14 year period Total 18 Mercurial poisons 6 Mercury & arsenic 1 Potassium dichromate 2 OrganoPhosphorous 5 Paraphenylenediamine / neem oil/ incense powder Bx showed ATN 3 / 18 died

43
Conclusions- Role of The Nephrologist
To expediate the excretion of toxin through normally functioning kidney To clear them through extracorporeal circulation To counter metabolic aberration To treat Acute Kidney Injury

44
PRECIOUS PAIR TAKE CARE

Similar presentations
 Department of Nephrology Jeong Kyung Hwan.>")


 는 14 일 농약을 마시고 자살을 기도해 병원 응급실로 후송됐으나 위 세척 등 모든 치료를 거부해.>")
 란 ? 1) 넓은 의미 order 문서보고 2) 좁은 의미 ; 1 시간 검사실 검체 접수 문서보고.>")

 발표자 : 김동원 2014. 04.>")
. 생명의 특징 (attributes of living matter) Six most important life processes Metabolism ( 신진대사 ) Responsiveness ( 반응, adaptation.>")











