Download presentation
Presentation is loading. Please wait.

1
Chap 2. 신경학적 검사

2
Clinical application of learning neuroscience
To understand the effects of nervous system lesions Signs and symptoms following a lesion of the nervous system depend on the location of the lesion Depending on their distribution - focal : limited to a single location - multifocal : limited to several, nonsymmetrical locations - Diffuse : affecting bilaterally symmetrical structures and does not cross the midline as a single lesion

3
Neurologic Evaluation
History Examination etiology Trauma Vascular disorders Inflammation Degenerative Neoplasm Immunologic Toxic or metabolic

4
History Speed of onset Pattern of progression Person’s mental status
Acute : indicating minutes or hours to maximal signs and symptoms Subacute : progressing to maximal signs and symtpoms over a few days Chronic : gradual worsening of signs and symptoms continuing for weeks or years Pattern of progression Person’s mental status Is the person awake? Is the person aware? Is the person able to respond appropriately to questions?

5
Headache Seizure and episodic loss of consciousness Visual disturbances Motor functions Sensory functions Cranial nerves function pain

6
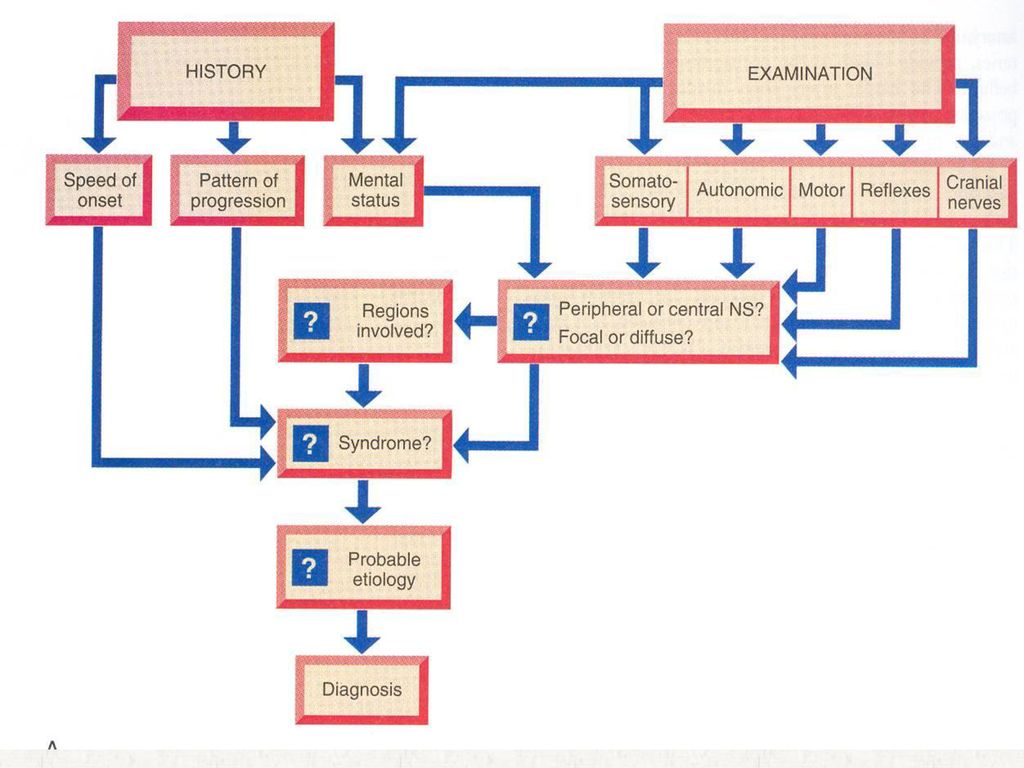
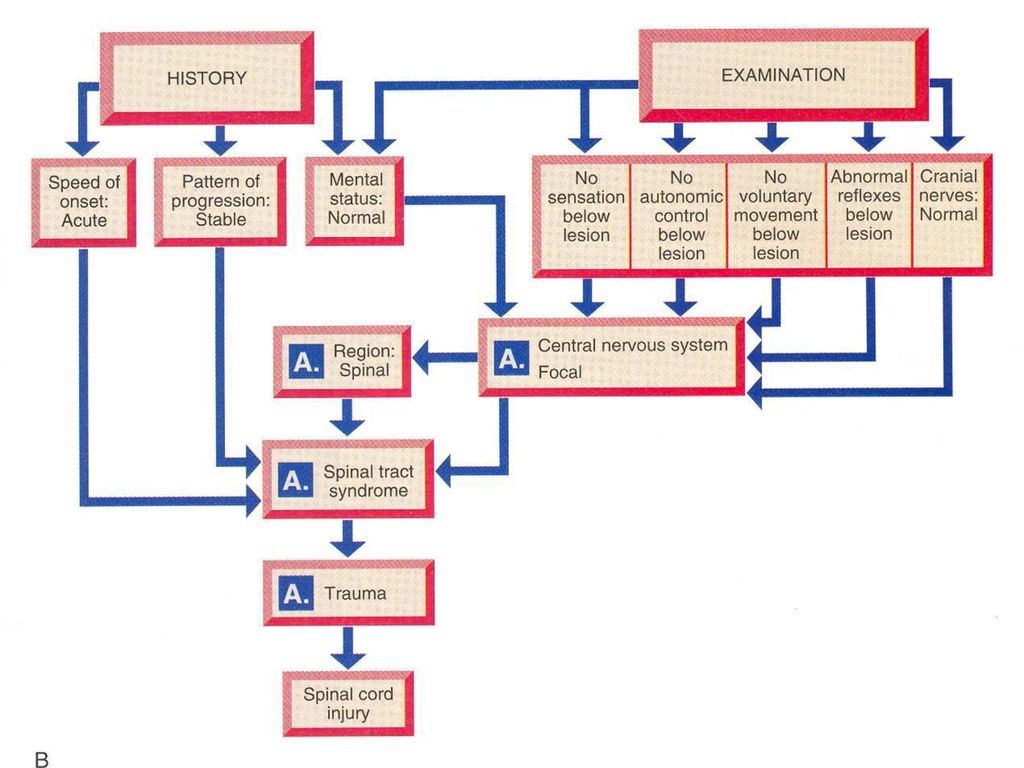
Examination Specific tests
to assess the function of sensory, autonomic , and motor systems Diagnosis : by synthesizing the information from the history and the examination Is the lesion in the peripheral or central nervous system? Is the lesion focal, multifocal, or diffuse? Does the pattern of signs and symptoms indicate a syndrome? What region or regions of the nervous system are involved? What is the probable etiology? What is the diagnosis?

9
Physical Examination The chief complaint History of present illness
Past history Family history Social history 순환기계, 호흡기계, 비뇨생식기계, 위장관계 및 골격계 체온, 맥박수, 호흡수, 혈압 머리, 목, 척추, 관절의 변형이나 운동 제한

10
Neurologic Examination
A. Cerebral function 1. General function a. General behavior b. consciousness: 뇌간의 망상조직 체계(reticular activating system)가 정상적인 의식을 유지하는데 관여함. - alert - drowsy - confusion - stupor - semi-coma - coma
가 정상적인 의식을 유지하는데 관여함. - alert. - drowsy. - confusion. - stupor. - semi-coma. - coma.")
11
c. orientation : time, space, person
d. mood e. language f. memory g. ability to acquire and manipulate knowledge - general information - similarities and differences - calculation - retention - right-left orientation - judgement - memory and comprehension h. Content of thought

12
1. Special function Aphasia Agnosia Apraxia

13
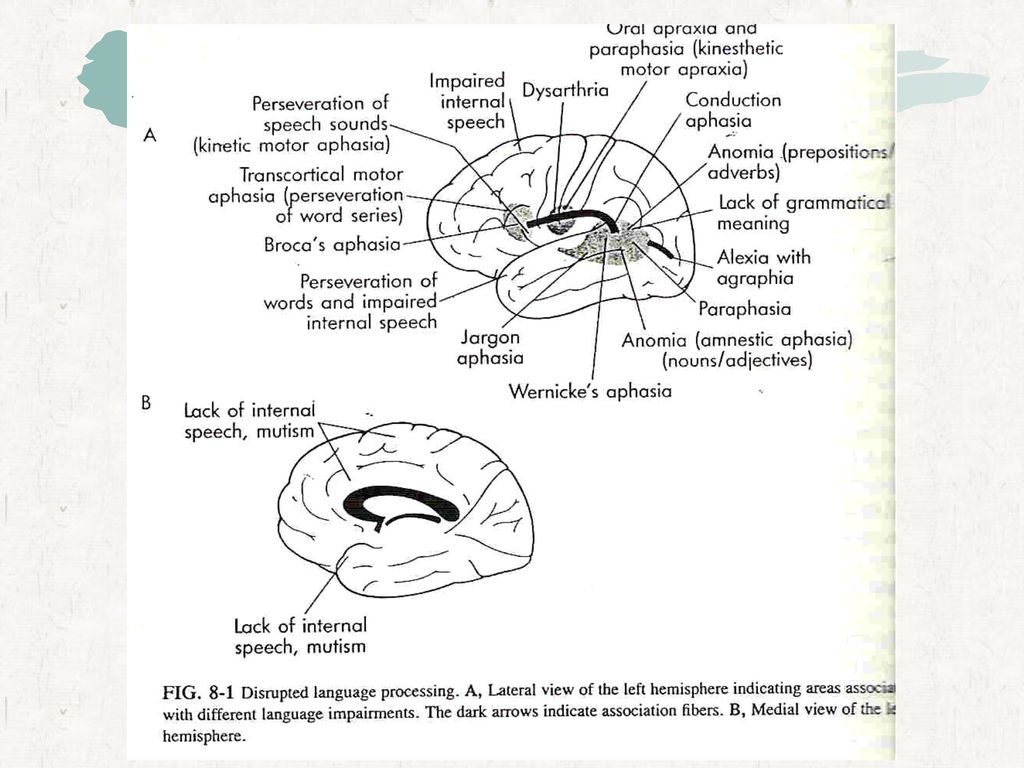
Language processing Wernicke aphasiatemporal Broca aphasiafrontal
Conductive aphasiaarcuate fasciculus Transcortical sensory aphasiaposterior occipitoparietal lobe Transcortical motor aphasiabroca area (partial involve) Anomic aphasia angular gyrus Global aphasiaWernicke+Broca
 Anomic aphasia angular gyrus. Global aphasiaWernicke+Broca.")
16
Aphasia (1)Expressive aphasia
- defect or loss in the power of expression by speech, writing, or gesture Oral expressive aphasia He knows what he wishes to say, but is unable to say it DDX: anarthria, dysarthria, agraphia, asymbolia, amimia

18
Anarthria- total loss of ability to articulate
Dysarthria-imperfect utterance of sound or words - phonation is preserved, but disease of the nerve to the organs of articulation interferes with clear enunciation Agraphia –loss of expression by writing Asymbolia amimia

19
-발성장애+정상적 기침=국소적 후두문제 또는 히스테리
-폭발성 기침이 아닌 둔감한 기침= 성대마비 -음성을 유지할 수 없고 피곤 = 중증근무력증 -어눌하고 술취한것 같다. -종종 말의 리듬이 깨진다. -알코올중독, 다별성경화증, 페니토닌중독 10 -단조롭고, 리듬이 없다 -말을 갑자기 시작하고 갑자기 끊는다 -파킨슨증. 12 7 -어눌하고 거의 입을 열수 없다. -가성뇌간마비, 운동신경원 병변

20
(2) Receptive aphasia - defect or loss of ability to comprehend spoken or written language or to interpret gestures visual receptive aphasia : loss of ability to comprehend the meaning or significance of printed or written word in the absence of actual loss of vision Area 18 : The patient sees the subjects but cannot identify them and react to them as a blind person would Area 19 : loss of ability to revisualize or to describe an object after it has been seen Area 39 : connected with striate cortex essential for the recognition and interpretation, and recall of the visual symbols of language : written and printed words have no meaning, although the patient may talk without difficulty and understand what is said to him

23
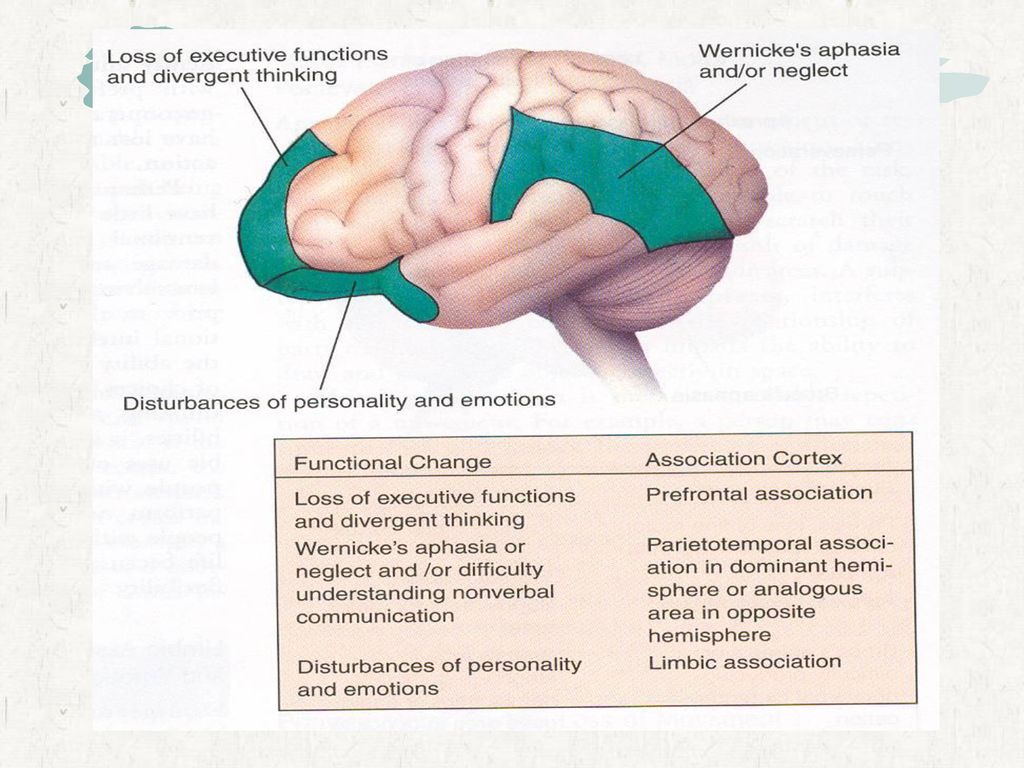
Auditory receptive aphasia(auditory sensory aphasia, auditory agnosia, Wernicke’s aphasia) : loss of ability to comprehend the significance of spoken words in the absence of deafness Lesion in the Heschl’s convolution (Area 41, 42) Transverse temporal gyri on the dorsal surface of posterior portion of the superior temporal convolution He can read without difficulty and may be able to speak normally but the loss of ability to comprehend the significance of spoken words includes those spoken by the patient himself as well as others.
 Transverse temporal gyri on the dorsal surface of posterior portion of the superior temporal convolution. He can read without difficulty and may be able to speak normally but the loss of ability to comprehend the significance of spoken words includes those spoken by the patient himself as well as others.")
24
(3) Expressive-receptive aphasia
- combination of the expressive and receptive aphasia Global or total aphasia, or central aphasia Most frequently encounted in clinical pracitice Extensive cortical lesions or subcortical damage with interruption of the association pathways (4) Amnesic Ahasia(anomia) Difficulty in evoking the names for subjects conditions, or qualities, with serious limitation in speaking and writing Lesion in the posterior temporal region between Wernicke’s area and the angular gyrus Diffuse rather than focal lesion
 Amnesic Ahasia(anomia) Difficulty in evoking the names for subjects conditions, or qualities, with serious limitation in speaking and writing. Lesion in the posterior temporal region between Wernicke’s area and the angular gyrus. Diffuse rather than focal lesion.")
25
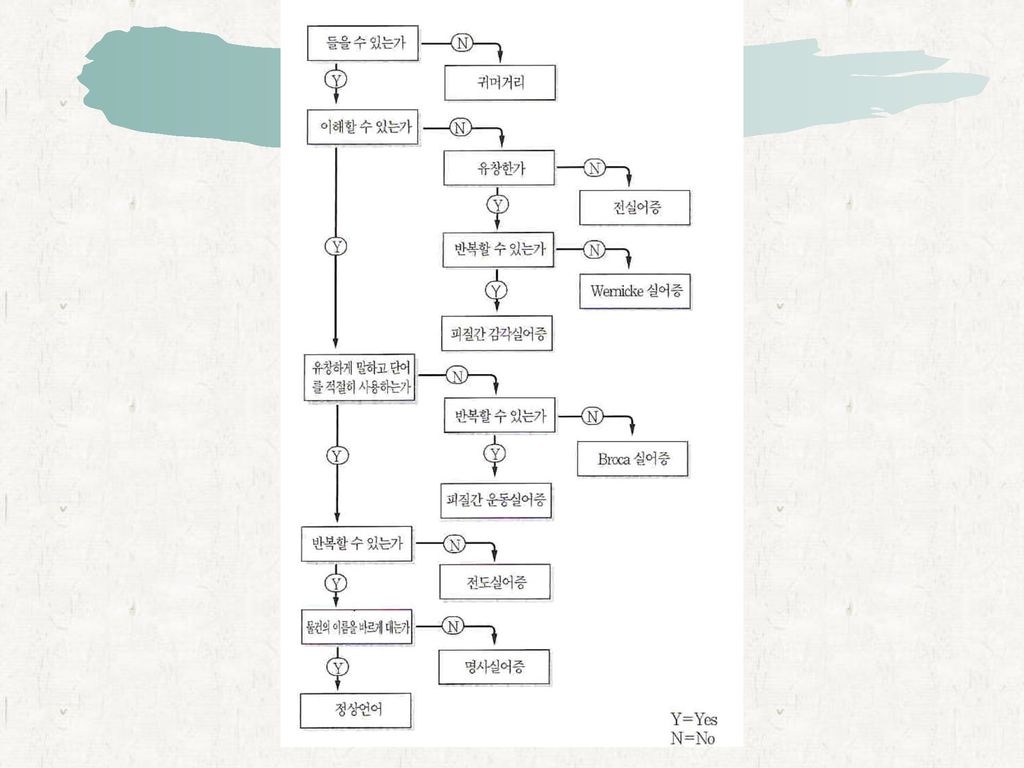
Classification of Aphasia

27
Agnosia Loss of the ability to comprehend the meaning or to recognize the importance of various types of stimulation Visual agnosia : fail to recognize the objects which the patient clearly sees. Lesion in the left parieto-occipital region Auditory agnosia : fail to recognize sounds in a patient who is nevertheless not deaf. Lesion in the left temporal lobe Asterognosis: loss of power to perceive the shape and nature of superficial contact in the absence of any sensory defect. Lesion in the parietal lobe, princially in the cortex of the posterior portions and the superior parietal lobule Anosognosia : ignorance of the existense of disease. Lesion in the nondominant parietal lobe. Lesion in the thalamoparietal pathways or the cortex bordering on the interparietal sulcus

28
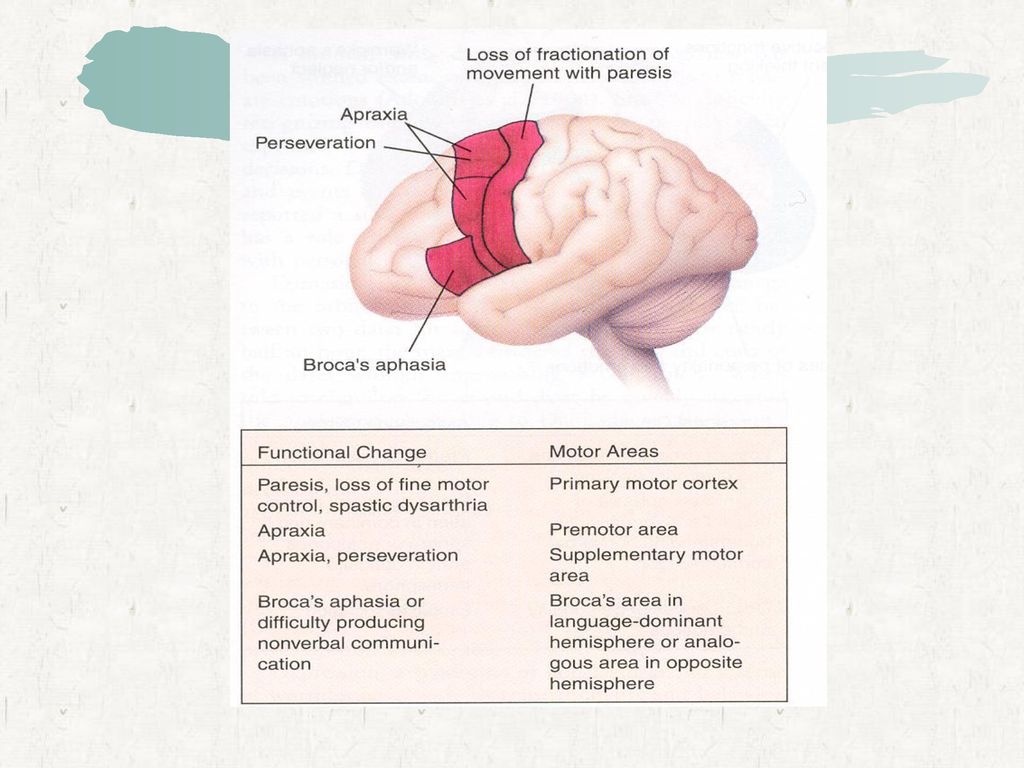
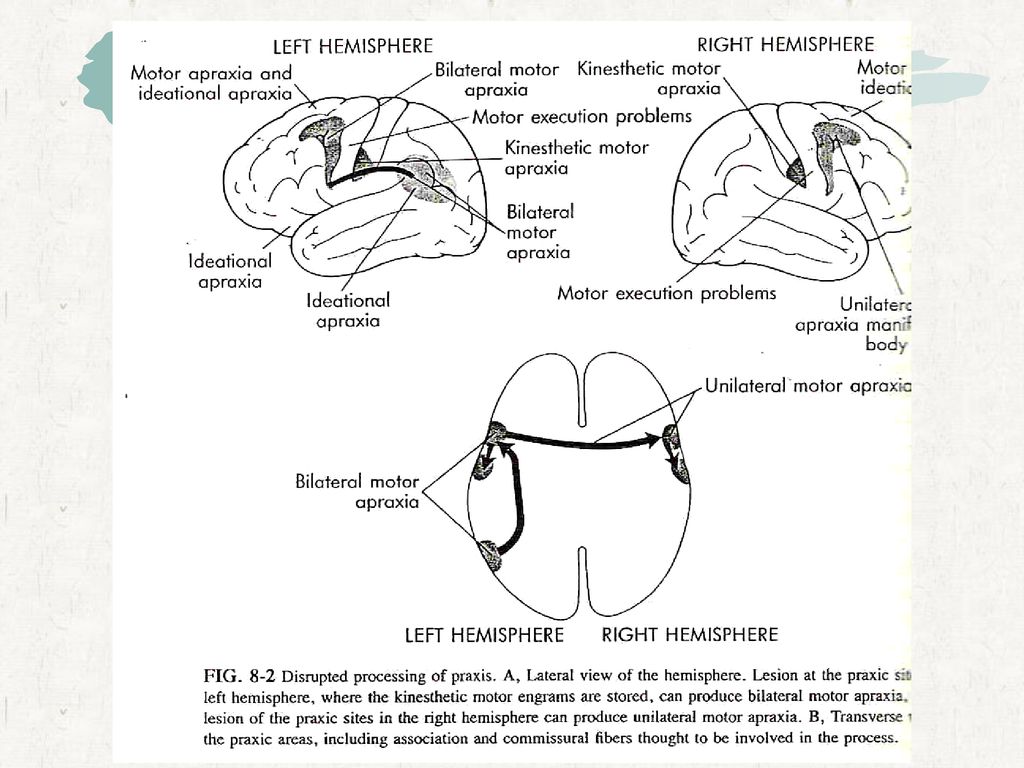
Apraxia :Defect in the ability to carry out purposive, useful or skilled acts, especially if compliance

30
Apraxia Kinectic, or motor apraxia: no motor weakness. Extremity can be used for unconscious. Movement. Inability for deliberate, purposeful acts. Lesions in the precentral or premotor cortex(area 4 or 6) Identical or sensory, apraxia : loss of ability to formulate the idealtional plan which is necessary for executing the several components of a complex acts. Simple and isolated movements are normal component parts may be executed properly, but they cannot be synthesized into a purposeful plan
 Identical or sensory, apraxia : loss of ability to formulate the idealtional plan which is necessary for executing the several components of a complex acts. Simple and isolated movements are normal component parts may be executed properly, but they cannot be synthesized into a purposeful plan.")
31
2. Cranial nerve function
Olfactory nerve : the sense of smell such as tobacco, coffee, menthol and perfume Optic nerve a. visual activity : snellen’s chart b. visual field : confrontation test c. light reflex 3. Oculomotor, trochlear and abducens nerve : 안구의 움직임 4. Trigeminal nerve a. sense to face b. corneal reflex c. motor

32
5. Facial nerve a. facial expressive muscles b. special sense of tongue 6. Vestibulocochlear nerve a. cochlear N : air conduction, bony conduction, audiometry b. vestibular N : calory test 7. Glossopharyngeal and vagus nerve a. gag reflex b. palatal reflex c. swallowing 8. Accessory nerve a. trapezius and sternocleidomastoid muscles 9. Hypoglossal nerve a. tongue muscles

33
3. Cerebellar function Function : equilibrium, muscle tone, coordination of voluntary movement Test : 1. simple walking test 2. romberg test 3. finger to nose test 4. heel to thin test 5. rapid alternating movement

34
A. Simple walking test 자세(posture) 보행(gait)
자율운동(coordinated automatic movements) 직선을 따라 걸을 수 있는 능력 걷다가 재빨리 돌 수 있는 능력 환자가 두발을 잇달아 걸을 수 있는지 검사 발 위치와 보행에 관한 모든 것
 직선을 따라 걸을 수 있는 능력. 걷다가 재빨리 돌 수 있는 능력. 환자가 두발을 잇달아 걸을 수 있는지 검사. 발 위치와 보행에 관한 모든 것.")
35
-근위부근육마비, 고관절의 양측성선천성탈골
-파킨슨병, 항우울제 뇌성마비, MS, 척수압박 -약물, 알코올, MS, 뇌혈관질환 -말초성 신경증, 후척수증상실 -근위부근육마비, 고관절의 양측성선천성탈골

36
B. Romberg test 눈을 감은 채 발꿈치와 발끝을 모두 바닥에 접촉한 상태로 서 있게 함 몸 흔들림의 증가는 소뇌나 안뜰 계통에 이상이 있는 환자에서 나타남 척수의 뒤기둥(posterior column)에 질환이 있는 환자눈을 뜨고는 자세를 잘 유지 하지만 눈을 감으면 넘어질 수 있음: 감각실조증(sensory ataxia) 흔한원인: 척수압박(경추 척수증, 종양) 드문원인: 매독성 척수증, 비타민 B12 결핍, 퇴행성 척수질환 눈을 뜨고 있는데도 균형을 유지 못하면: 흔한원인: 소뇌 병변과 중추 및 말초 전정계 증후군 심한불안정 소뇌성 실조증(cerebellar ataxia)앞뒤로 흔들림
에 질환이 있는 환자눈을 뜨고는 자세를 잘 유지 하지만 눈을 감으면 넘어질 수 있음: 감각실조증(sensory ataxia) 흔한원인: 척수압박(경추 척수증, 종양) 드문원인: 매독성 척수증, 비타민 B12 결핍, 퇴행성 척수질환. 눈을 뜨고 있는데도 균형을 유지 못하면: 흔한원인: 소뇌 병변과 중추 및 말초 전정계 증후군 심한불안정. 소뇌성 실조증(cerebellar ataxia)앞뒤로 흔들림.")
37
C. Finger to nose test 환자에게 손가락 끝을 환자의 코 위에 놓은 다음 팔 길이 정도로 떨어져 위치하는 검사자의 손가락에 닿도록 함 Finger to finger test: 환자의 두 팔을 앞쪽으로 뻗게 한 뒤에 양쪽 집게손가락 끼리 마주치게 함목표물을 지나쳐 버리면 dysmetria 소뇌질환

38
불수의적 과잉운동 때문에 느리게 뒤틀리며 특히 손과 손목에서 심하다.
-불수의적 운동이 특히 어깨나 골반의 근육에서 시작하여 내던지는 듯하거나 거칠게 내뻗는 듯한 행동으로 나타남. 불수의적 과잉운동 때문에 느리게 뒤틀리며 특히 손과 손목에서 심하다. -짧고 빠른 불수의적 경련이 한 근육에서 나타나 때로는 수의적 운동처럼보이는 여러 형태의 움직임을 보여준다. -주동근과 길항근이 같이 수축해서 비정상적인 자세를 취한다. 유지되는 형태는 극단적 신전과 굴곡이다.

39
D. Heel to Thin test 한쪽 발꿈치를 다른 쪽 무릎에 닿게 한 다음 발꿈치를 정강이 앞부분 아래로 서서히 내려 발목까지 이르도록 지시함 목표물을 지나쳐 버리는 겨냥이상은 소뇌질환

40
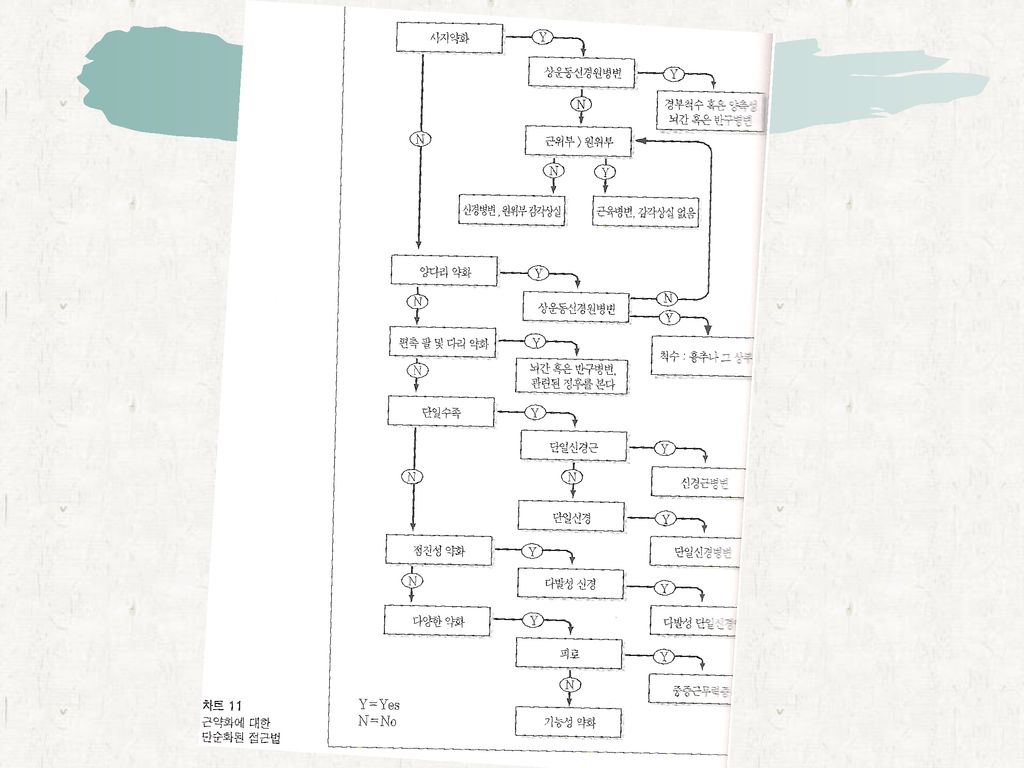
4. Motor function Tone : flaccidity, spasticity, rigidity
Involuntary movement Power of muscle 0 : no contraction 1 : trace of contraction 2 : active movement, with gravity eliminated 3 : active movement against gravity 4 : active movement against gravity and resistance 5 : normal

41
상위운동신경원 증후군과 하위운동신경원 증후군의 비교
상위운동신경원 증후군과 하위운동신경원 증후군의 비교 Upper motor nueron Lower motor neuron Type of paralysis 강직성 부전마비 (spastic paresis) 이완성 마비 (flaccid paralysis) Atrophy 거의 없음 심한 근위축 Deep tendon reflex 항진 감소 또는 소실 Pathological reflex Babinski sign이 나타남 나타나지 않음 Superficial reflex 감소 증가 fibrillation 없음 있음
 이완성 마비. (flaccid paralysis) Atrophy. 거의 없음. 심한 근위축. Deep tendon reflex. 항진. 감소 또는 소실. Pathological reflex. Babinski sign이 나타남. 나타나지 않음. Superficial reflex. 감소. 증가. fibrillation. 없음. 있음.")
43
5. REFLEX Deep tendon reflex - biceps reflex - triceps reflex
- knee reflex - ankle reflex B. Superficial reflex - abdominal reflex - cremasteric reflex - plantar reflex - clonus 0: 움직임이 없을때, +1: 약한반응을 나타낼때, +2: 정상일때, +3: 강한반응을 나타낼때, +4: 간대성 경련이 있을때

44
6. Sensory function Pain : 핀으로 찌르는 자극이나 강하는 누루는 자극을 알아차리는지 검사
Temperature: 따뜻한 것과 찬 것을 알아내고 구분하는 능력 Touch: 솜으로 피부를 가볍게 문질러 보고 이를 감지할 수 있는지 검사 Vibration: 환자의 뼈 돌출부에 소리굽쇠를 갖다대고 진동감각을 감지할 수 있는지 Sense of position : 위치의 감각 Stereognosis: 사물의 형태, 크기 및 무게를 인지하는 능력을 검사하기 위해 환자의 손에 올려놓고 알아 맞추게 함 Two-point discrimination: 콤파스나 캘리퍼를 이용하여 서로 떨어져 있는 피부 위 두 지점을 자극했을때, 두 점에 가해진 자극이 마치 한 개의 점으로 인지되는 최단거리(손가락끝 : 0.3~0.6㎝, 손바닥 및 발바닥: 1.5~2㎝, 손등: 3㎝, 정강이: 4㎝) Topognosis : 눈을 감은뒤 환자에게 접촉된 지점을 지적하게 함
 Topognosis : 눈을 감은뒤 환자에게 접촉된 지점을 지적하게 함.")
45
Examining Neonates General status Neurologic examination 뇌신경
A. optic nerve : 영아가 빛에 반응하여 눈을 깜박이는지 검사 B. oculomotar N, trochlear N, abducens N. : 양쪽 동공의 크기, 모양 그리고 빛에 대한 동공 반사, 머리를 바깥쪽으로 회전시키면 그와 반대쪽으로 양쪽 눈이 돌아감 C. trigeminal N, facial N. : 손가락이나 유두를 영아의 양 입술 사이에 접촉시키면 빨기반사(sucking reflex)가 유발, 포유반사(rooting reflex)는 손가락 끝으로 영아의 볼을 자극하면 영아의 입이 벌어지고 자극 받은 방향으로 얼굴을 돌리는 반사 D. vestibulocochlear N.: 큰소리에 대해 눈을 깜박거리는 반응, 미로반사(labyrinthine reflex)를 검사할때, 검사자는 영아를 안고 오른쪽으로 여러 번 회전한다음 왼쪽으로 여러 번 회전한다. 정상 영아는 회전하는 방향으로 앞쪽을 바라보고, 회전하는 것을 멈추면 영아는 회전하는 반대방향으로 뒤쪽을 쳐다본다 E. glossophangeal N. : 영아의 연하능력
가 유발, 포유반사(rooting reflex)는 손가락 끝으로 영아의 볼을 자극하면 영아의 입이 벌어지고 자극 받은 방향으로 얼굴을 돌리는 반사. D. vestibulocochlear N.: 큰소리에 대해 눈을 깜박거리는 반응, 미로반사(labyrinthine reflex)를 검사할때, 검사자는 영아를 안고 오른쪽으로 여러 번 회전한다음 왼쪽으로 여러 번 회전한다. 정상 영아는 회전하는 방향으로 앞쪽을 바라보고, 회전하는 것을 멈추면 영아는 회전하는 반대방향으로 뒤쪽을 쳐다본다. E. glossophangeal N. : 영아의 연하능력.")
46
운동계와 반사 A. incurvation reflex B. muscle tone C. limb motion D. joint motion E. grasp reflex F. traction responses G. stepping responses H. placing and supporting reaction 감각계

47
신경계 영상진단 검사와 실험실 검사의 역할 신경 영상 연구 : X선, 혈관촬영술, 척수조영술, 컴퓨터 단층촬영(CT), 자기공명영상(MRI) 뇌척수액 검사 :요추천자 전기 생리검사 : 뇌파(EEG), 유발전위(evoked potential), 근전도(EMG), 신경전도검사
, 유발전위(evoked potential), 근전도(EMG), 신경전도검사.")
48
X-선 촬영술 머리뼈 골절 및 머리뼈의 가능한 함몰 정도를 알아내거나 머리뼈와 관련되어진 석회화된 뇌의 병소, 이물질 또는 종양 기뇌조영술: 간질, 뇌위축 및 선천성 뇌병소를 가진 환자 혈관조영술 : 혈관의 폐쇄, 기형 및 동맥류가 의심되는 경우 두개내압과 관련되어 혈관의 위치가 정상적인지 병적으로 변화되었는지를 결정 넙다리 동맥으로 삽입된 도관을 통해 들어간 조영물질을 보여주는 연속적인 X선상으로 구성됨

49
전산화단층촬영술(computed tomogrpahy)
머리뼈, 뇌, 뇌실, 수조, 큰혈관의 횡단면 비정상적인 석회화, 뇌부종, 수두증, 많은 형태의 종양 및 낭, 출혈, 큰대동맥류, 혈관기형 자기공명영상(MRI : magnetic resonance imaging) - 몸이나 뇌의 얇은 조각 내에 수소처럼 홀수 번호를 가진 양성자 원소들의 공간적 분포는 외부의 라디오 주파 수신호에 대한 원소의 반응에 의해 결정
 - 몸이나 뇌의 얇은 조각 내에 수소처럼 홀수 번호를 가진 양성자 원소들의 공간적 분포는 외부의 라디오 주파 수신호에 대한 원소의 반응에 의해 결정.")
50
뇌파검사(Electrocephalography)
뇌의 진행적이며 자발적인 전기적 활동을 연구하는 비 침해적인 방법 뇌의 구조적 질병 특히 경련성 질환을 분류 유발전위(evoked potentials) 뇌파는 지속적 또는 자발적 전기활동을 기록하는 반면에 유발전위 기록은 다양한 감각경로의 자극에 반응하는 대뇌겉질 감각영역과 겉질 아래의 중계핵의 활동을 기록 근전도검사(electromyography) 휴식때의 근육과 활동적으로 수축할때 나타나는 전기 활동의 연구 신경전도검사(nerve conduction studies) - 피부를 통하여 말초신경을 자극하고 근육과 감각신경 활동전위를 기록함으로써, 전도 속도와 원위부 잠복기 및 반응의 진폭을 조사하여 말초신경병변에 대한 중요한 정보를 제공
 뇌파는 지속적 또는 자발적 전기활동을 기록하는 반면에 유발전위 기록은 다양한 감각경로의 자극에 반응하는 대뇌겉질 감각영역과 겉질 아래의 중계핵의 활동을 기록. 근전도검사(electromyography) 휴식때의 근육과 활동적으로 수축할때 나타나는 전기 활동의 연구. 신경전도검사(nerve conduction studies) - 피부를 통하여 말초신경을 자극하고 근육과 감각신경 활동전위를 기록함으로써, 전도 속도와 원위부 잠복기 및 반응의 진폭을 조사하여 말초신경병변에 대한 중요한 정보를 제공.")
Similar presentations







 주요 내용 소개>")









 Brain CT 건국대학교 충주병원 영상의학과>")



