Download presentation
Presentation is loading. Please wait.

1
방사선 과연 우리의 친구인가 ? 경 희 의 대 황보 영

2
Radiation Hazard

3
X-ray & Roentgen.

4
Contents 질병 적용 및 우리 병원 Data 국제 권고 기준 방사선 피폭의 해로움 방사선의 의료 이용 방사선의 정의 및 의의, 이용 현황

5
방사선 이란 ? 정의 에너지가 높아 불안한 상태에 있 는 원자 또는 원자핵이 안정된 상 태를 찾기 위해 방출하는 에너지 의 흐름 종류 태양 자외선, 적외선, microwave, radio wave, ionizing radiation

6
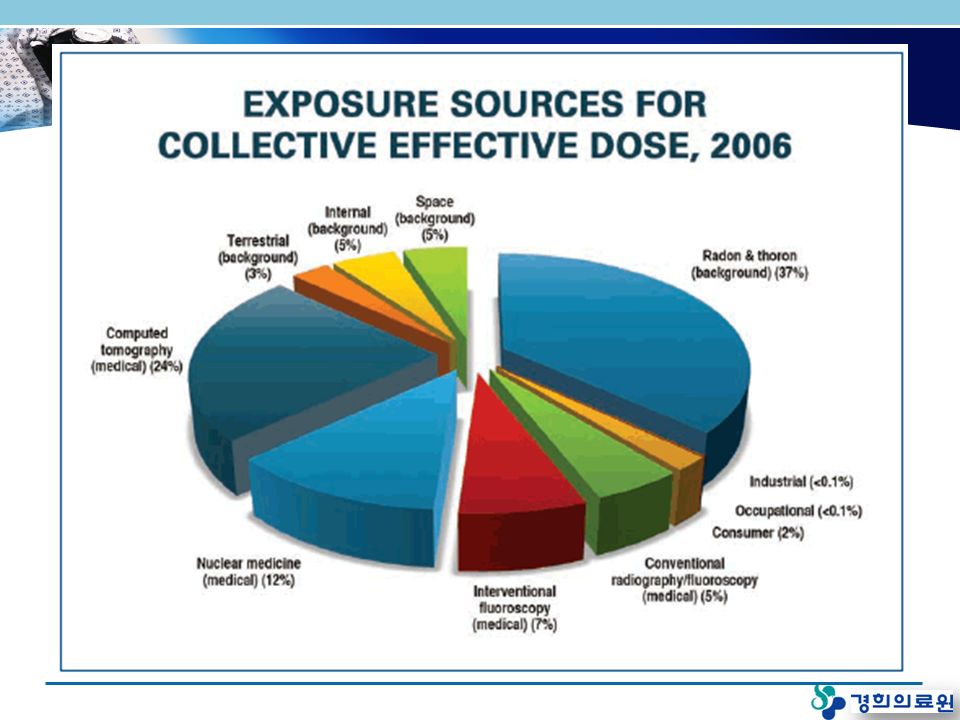
일상생활에서 방사선 노출 방사선은 우주가 생겨날 때부터 존재 우리는 생활하는 동안 항상 환경 중의 방사선에 노출 미국 : 방사선으로 인한 연간유효선량은 3.6mSv 정도로 평가 음식물, 담배 등 에 함유된 소량의 방사성물질 호흡을 통해 흡입되는 라돈 의료과정 ( 진단용 엑스선 촬영과 방사선 치료등 ) 에서의 인공방사선 연기감시기, 건축자재 속의 방사성물질
 에서의 인공방사선 연기감시기, 건축자재 속의 방사성물질")
7
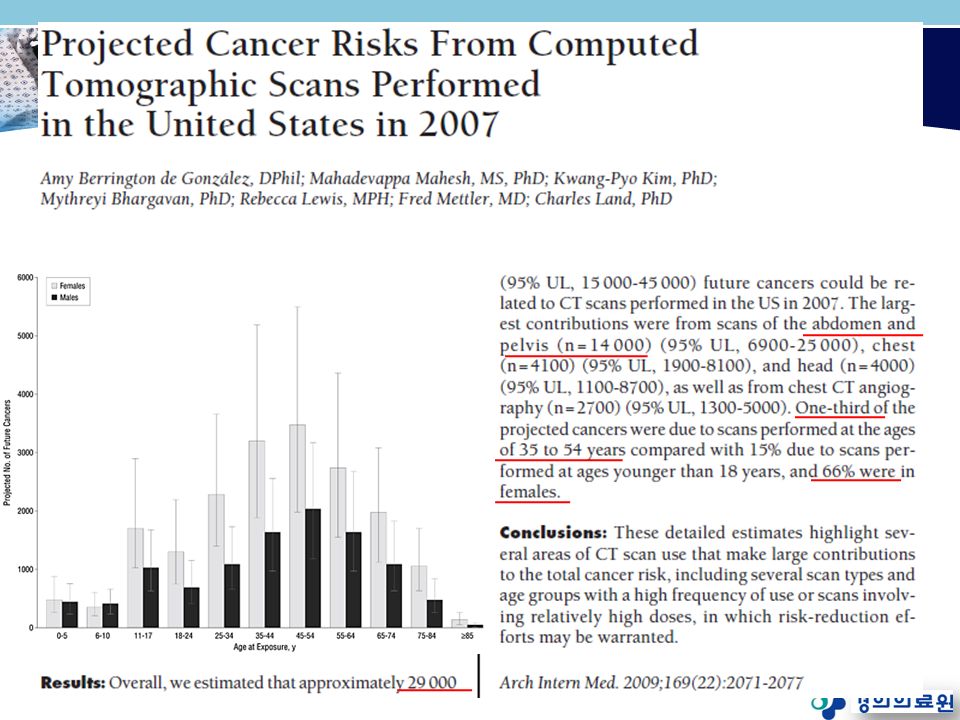
증가하는 방사선량 ICRP( 국제 방사선 방어 위원회 ) International Commission on Radiological Protection 엑스선 검사 횟수 20 억 회 이상 (1995 년 전 세계 ) 인공 방사선 15% 이중 의료에서 피폭 80~90% 미국 2007 년 : CT 93 년에 비해 3 배 증가, 7000 만 /yr –Arch of Int Med 2009 우리나라 CT 촬영건수 270 만건 (2006) CT 보급 : 915 대 (1995) 2347 대 (2007) 4.7 배 증가 – 건강보험심사평가원 2007
 International Commission on Radiological Protection 엑스선 검사 횟수 20 억 회 이상 (1995 년 전 세계 ) 인공 방사선 15% 이중 의료에서 피폭 80~90% 미국 2007 년 : CT 93 년에 비해 3 배 증가, 7000 만 /yr –Arch of Int Med 2009 우리나라 CT 촬영건수 270 만건 (2006) CT 보급 : 915 대 (1995) 2347 대 (2007) 4.7 배 증가 – 건강보험심사평가원 2007")
8
검사 범주별 전 세계 연간 의료 X 선 사용 UNSCEAR, 2000 Contribution to frequencyContribution to collective dose

9
CT 사용량의 증가 ( 미국 ) N Engl J Med 2007;357.
 N Engl J Med 2007;357.")
11
전국 CT 설치 현황 (2007)
")
12
CT 검사 횟수 현황 출처 : 건강보험심사평가원 자료

13
Contents 질병 적용 및 우리 병원 Data 국제 권고 기준 방사선 피폭의 해로움 방사선의 의료 이용 방사선의 정의 및 의의, 이용 현황

14
방사선 용어 1 (1) 조사선량 (Exposure Dose, X) 단순히 공간상의 어떤 위치에서 방사선 강도의 세기를 나타내는 단위 : 렌트겐 (R) (2) 흡수선량 (Absorbed Dose, D) 방사선이 지나는 곳에 어떤 물체가 있음 이때 노출 ( 피폭 ) 된 양 물질 단위질량 (1kg) 당 흡수된 방사선 에너지량 (J) 조직 / 장기의 방사선 위험을 평가하는 기본 양으로 사용 전통적인 단위 : 라드 (rad), SI 단위 : 그레이 (Gy) 1Gy = 1J/kg = 100rad
 조사선량 (Exposure Dose, X) 단순히 공간상의 어떤 위치에서 방사선 강도의 세기를 나타내는 단위 : 렌트겐 (R) (2) 흡수선량 (Absorbed Dose, D) 방사선이 지나는 곳에 어떤 물체가 있음 이때 노출 ( 피폭 ) 된 양 물질 단위질량 (1kg) 당 흡수된 방사선 에너지량 (J) 조직 / 장기의 방사선 위험을 평가하는 기본 양으로 사용 전통적인 단위 : 라드 (rad), SI 단위 : 그레이 (Gy) 1Gy = 1J/kg = 100rad")
15
방사선 용어 2 (3) 유효선량 (Effective Dose, ED) 인체 내부에는 다양한 장기나 조직들이 있는데 같은 방사선량 ≠ 같은 위험도 같은 선량에서도 인체 조직이 처하는 위험의 차이를 반영하기 위해 상대적 방사선 위험을 비교하는 지표로 사용 측정단위 sievert (Sv), rem; 100rem=1Sv
 유효선량 (Effective Dose, ED) 인체 내부에는 다양한 장기나 조직들이 있는데 같은 방사선량 ≠ 같은 위험도 같은 선량에서도 인체 조직이 처하는 위험의 차이를 반영하기 위해 상대적 방사선 위험을 비교하는 지표로 사용 측정단위 sievert (Sv), rem; 100rem=1Sv")
16
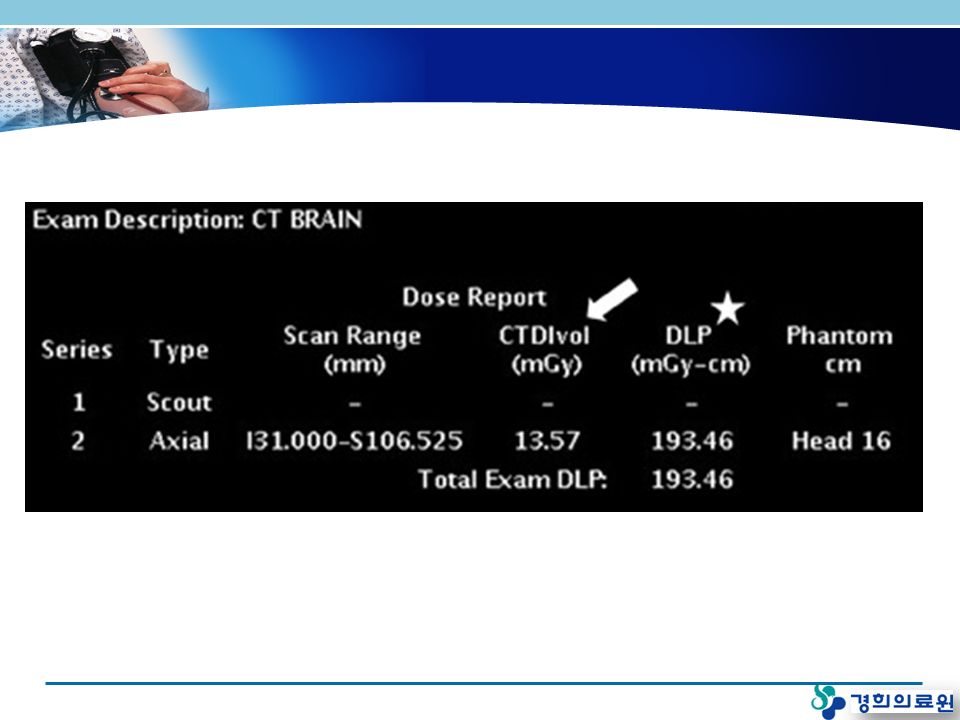
CT Dose Report ?

17
방사선 용어 3 CTDI : CT dose index (CT 선량지수 ) – 단일 슬라이스 scan 에서 방사선값, mGy 로 표시 –CT 선량측정용 표준 모의피폭체 ( 팬텀 ) 에서 측정 DLP : dose length product 선량길이곱 – 모든 영상에 대한 총 선량의 측정값 –CTDI 에 스캔한 길이를 곱함 –DLP (mGy ∙ cm) =CTDIvol ∙ scan length 유효선량 (mSv) –DLP ∙ Conversion coefficiency
 – 단일 슬라이스 scan 에서 방사선값, mGy 로 표시 –CT 선량측정용 표준 모의피폭체 ( 팬텀 ) 에서 측정 DLP : dose length product 선량길이곱 – 모든 영상에 대한 총 선량의 측정값 –CTDI 에 스캔한 길이를 곱함 –DLP (mGy ∙ cm) =CTDIvol ∙ scan length 유효선량 (mSv) –DLP ∙ Conversion coefficiency")
19
유효선량 구하기

20
CT Dose Report (KHMC) Effective dose= DLP x con factor 1508.96 x 0.015 = 22.63 mSv
 Effective dose= DLP x con factor x = mSv")
21
우리의 무지함 Radiology 2004;231:393-8

22
Typical Radiation Dose N Engl J Med 2007;357

23
Diagnostic Procedure Typical Effective Dose (mSv) 1 Number of Chest X rays (PA) for Equivalent Effective Dose 2 Time Period for Equivalent Effective Dose from Natural Background Radiation 3 Chest x ray (PA )0.0212.4 days Skull x ray0.1512 days Lumbar spine1.575182 days I.V. urogram31501.0 year Upper G.I. exam63002.0 years Barium enema84002.7 years CT head2100243 days CT abdomen105003.3 years

24
Radiation dose of various exam Am J Gastroenterol 2008;103

25
Radiation dose of various CT Arch Intern Med. 2009;169(22) 31mSv
 31mSv")
26
Contents 질병 적용 및 우리 병원 Data 국제 권고 기준 방사선 피폭의 해로움 방사선의 의료 이용 방사선의 정의 및 의의, 이용 현황

27
Radiation Sensitive Organ

28
Radiation & Ca Risk?

29
Radiation Hazard of CT N Engl J Med 2007;357.

30
JAMA. 2007;298(3):317-323 Radiation dose 남자 : 15~23 mSv 여자 : 19~29 mSv 20 세 여자 : 0.70% 40 세 여자 : 0.35%
: Radiation dose 남자 : 15~23 mSv 여자 : 19~29 mSv 20 세 여자 : 0.70% 40 세 여자 : 0.35%.")
31
Excess Cancer Mortality Am J Roentegenol 2007

32
위험도 상대 비교 건강상의 리스크평균수명손실 직업의 종류평균수명손실 하루에 20 개피흡연 6년6년 모든 산업 60 일 과체중 (15%)2년2년 농업 320 일 음주 ( 미국 평균 )1년1년 건설업 227 일 모든 사고 207 일 광산 및 채석장 167 일 자연재해 7일7일 제조업 40 일 직업적 피폭 (10mSv)51 일 직업적 피폭 (10mSv)51 일
2년2년 농업 320 일 음주 ( 미국 평균 )1년1년 건설업 227 일 모든 사고 207 일 광산 및 채석장 167 일 자연재해 7일7일 제조업 40 일 직업적 피폭 (10mSv)51 일 직업적 피폭 (10mSv)51 일")
34
Arch Intern Med 2009;169

35
Contents 질병 적용 및 우리 병원 Data 국제 권고 기준 방사선 피폭의 해로움 방사선의 의료 이용 방사선의 정의 및 의의, 이용 현황

36
CT 검사 환자선량 권고량 가이드라인 방사선안전관리시리즈 2009. 9

37
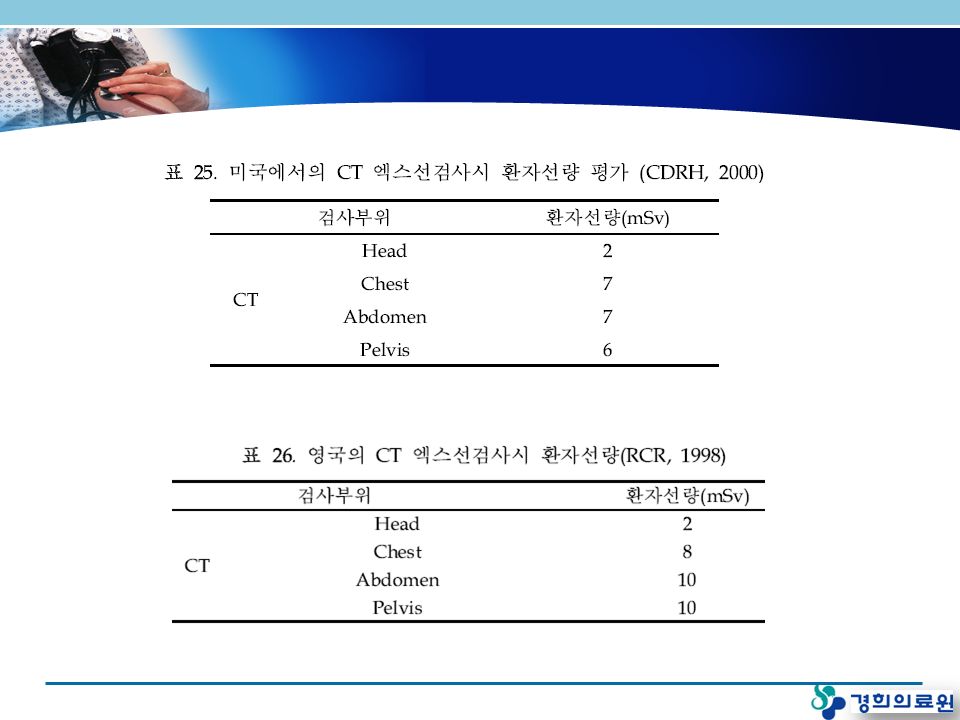
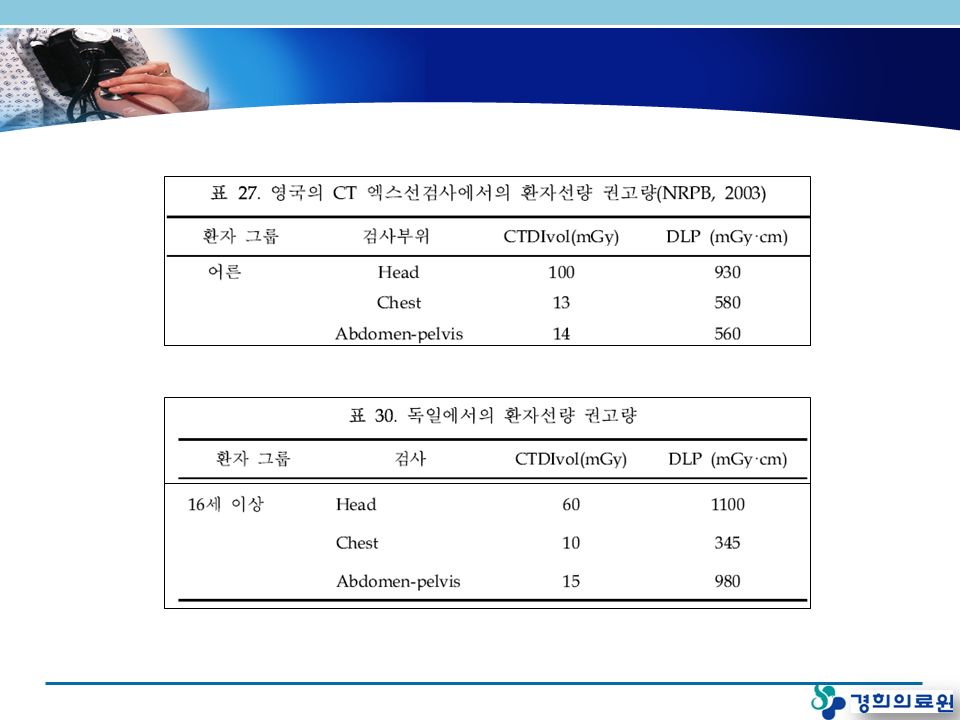
CT 엑스선검사에서의 환자선량 권고량 ICRP Supporting Guidance

40
우리나라 연구 - 방사선 평균치 전국 200 개 병원 - 복부 CT

41
Contents 질병 적용 및 우리 병원 Data 국제 권고 기준 방사선 피폭의 해로움 방사선의 의료 이용 방사선의 정의 및 의의, 이용 현황

42
Introduction CD & UC Chronic & Relapsing, life long disease Young age Inflammation in GI tract with multiple extraintestinal manifestation Radiologic imaging study Initial diagnosis Assessment of disease activity Evaluation of complications and extraintestinal manifestation Monitoring of response to therapy imaging study (CT, fluoroscopy, MRI, US, etc)
")
43
Radiation exposure in IBD Population-based Cohort study 1990 ~ 2001 215 IBD patients, Olmsted country, Minesota Median cumulative ED (mSv): CD=26.6, UC=10.5 Annual median ED (mSv/yr): CD=3.1, UC=1.2 Single center retrospective study 1992 ~ 2007 Ireland 409 CD patients Mean cumulative ED 36.1 mSv MDCT ↑, 2phase & 3phase dynamic abdominal CT ↑ Increased radiation dose Am J Gastroenterol 2008 Gut 2008;57:1524-29
: CD=26.6, UC=10.5 Annual median ED (mSv/yr): CD=3.1, UC=1.2 Single center retrospective study 1992 ~ 2007 Ireland 409 CD patients Mean cumulative ED 36.1 mSv MDCT ↑, 2phase & 3phase dynamic abdominal CT ↑ Increased radiation dose Am J Gastroenterol 2008 Gut 2008;57:")
44
Objectives Quantify the radiation dose in IBD patient –Cumulative ED, Annual median ED Analysis between CD and UC Examine patterns of use of diagnostic imaging Identify factors associated with exposure to high level of diagnostic radiation

45
Patients & Method Single tertiary center, retrospective study Study population 14 ~ 70 yr-old-age IBD patient 2000.1.1-2009.6.30 Kyung Hee University Medical center, GI department Over 6 months follow-up period CD 148, UC 256 patients 14 pt excluded due to lack of data Total CD 139, UC 251 patients were enrolled. Cumulative ED was calculated retrospectively based on all imaging study National Radiological Protection Borad estimated organ dose Abdominal CT median ED was calculated based on dose report

46
Table1. Patients and Disease Characteristics CT = computed tomography; ED = effective dose; mSv = millisieverts * Independet t-test

47
Table 2. Median effective dose of non-CT X-ray exams & percentage of patients who had each exam ExamED (mSv/study) CD patients (%)UC patients(%)P-value* Non GI studies Chest X-ray0.17114 (82.0)178 (70.9)0.016 KUB0.7223 (16.5)46 (18.3)0.659 IVP3.57 (5.0)9 (3.6)0.498 Spine1.527 (19.4)76 (30.3)0.020 Mammography34 (2.9)19 (7.5)0.060 BMD0.00812 (8.6)25 (10.0)0.668 Subclavian0.1717 (12.2)16 (6.4)0.047 GI studies Simple Abdomen0.36105 (75.5)105 (41.8)<0.001 Small bowel2.292 (66.2)5 (2.0)<0.001 Colon26 (4.3)14 (5.6)0.589 Pelvis0.7211 (7.9)26 (10.4)0.430 ERCP1.82 (1.4)2 (0.8)0.547 CT = computed tomography; ED = effective dose; mSv = millisieverts; KUB = kidney, ureter, bladder IVP = intra venous pyelography; BMD = bone mineral densitometry * P for difference between CD and UC, analysis by Chi square test
 CD patients (%)UC patients(%)P-value* Non GI studies Chest X-ray (82.0)178 (70.9)0.016 KUB (16.5)46 (18.3)0.659 IVP3.57 (5.0)9 (3.6)0.498 Spine1.527 (19.4)76 (30.3)0.020 Mammography34 (2.9)19 (7.5)0.060 BMD (8.6)25 (10.0)0.668 Subclavian (12.2)16 (6.4)0.047 GI studies Simple Abdomen (75.5)105 (41.8)<0.001 Small bowel2.292 (66.2)5 (2.0)<0.001 Colon26 (4.3)14 (5.6)0.589 Pelvis (7.9)26 (10.4)0.430 ERCP1.82 (1.4)2 (0.8)0.547 CT = computed tomography; ED = effective dose; mSv = millisieverts; KUB = kidney, ureter, bladder IVP = intra venous pyelography; BMD = bone mineral densitometry * P for difference between CD and UC, analysis by Chi square test.")
48
Table 3. Median effective dose of CT exams & percentage of patients who had each exam Exam ED (mSv/study) CD patients (%)UC patients(%)P-value Chest CT83 (2.2)18 (7.2)0.036 Brain CT27 (5.0)16(6.4)0.591 Abdominal CT22.26120 (86.3)99 (39.4)<0.001 139 회 Abdominopelvic CT 방사선 조사량측정 Median effective dose 22.26±7.28 (7.96~49.46) mSv
 CD patients (%)UC patients(%)P-value Chest CT83 (2.2)18 (7.2)0.036 Brain CT27 (5.0)16(6.4)0.591 Abdominal CT (86.3)99 (39.4)< 회 Abdominopelvic CT 방사선 조사량측정 Median effective dose 22.26±7.28 (7.96~49.46) mSv.")
49
Number of abdominal CT

50
Fig. 1. Contribution to the cumulative effective dose in CD patients

51
Fig. 2. Number of IBD patients according to cumulative effective dose (CED) of diagnostic radiation CED > 50 mSv CD = 47(34%) UC = 23( 9% )
 of diagnostic radiation CED > 50 mSv CD = 47(34%) UC = 23( 9% ).")
52
Fig. 3. Cumulative effective dose differences between sub- groups in CD (Montreal classification) Age at diagnosis Disease location Upper GI involve Disease behavior Perianal involve p=0.720p=0.089p=0.581p=0.029p=0.118 All
 Age at diagnosis Disease location Upper GI involve Disease behavior Perianal involve p=0.720p=0.089p=0.581p=0.029p=0.118 All.")
53
Fig. 4. Cumulative effective dose differences between sub-groups in CD SurgeryAdmissionInfliximabAZA/6MPIV steroid p<0.001 p=0.028p=0.163p=0.157 All

54
Fig. 5. Cumulative effective dose differences between sub-groups in UC Disease extent Surgery Admission IV steroid AZA /6MP Infliximab p<0.001 p=0.890p=0.207p=0.249 All

55
Summary Significant diagnostic radiation exposure in IBD patinent. Radiation exposure in CD patients was significantly higher than in UC patients. Some patients with very high exposure (>50 mSv) Factor associated with high ED –CD: stricturing, penetrating disease, Infliximab, surgery, admission –UC: pancolitis, surgery, admission High level of radiation exposure was mainly due to use of CT.
 Factor associated with high ED –CD: stricturing, penetrating disease, Infliximab, surgery, admission –UC: pancolitis, surgery, admission High level of radiation exposure was mainly due to use of CT..")
56
Conclusions A considerable number of IBD patients are at risk of exposure to significant amount of diagnostic radiation. A considerable number of IBD patients are at risk of exposure to significant amount of diagnostic radiation. The preferential use of nonradiation-based investigation may be the solution. The preferential use of nonradiation-based investigation may be the solution. After careful consideration, decide to take a CT exam. Need to apply a low-radiation protocol at CT exam.

57
Benefit Diagnosis Comfortable Noninvasive Fast Painless CT 1. CT protocol low dose 2. 의사 및 환자 교육 : 방사선의 위험성 인식 3. 의사 : 꼭 필요한지 생각 4. 대체 영상 진단법의 사용 Harm Radiation Cancer risk Conclusions

Similar presentations


 이용 가능한 template.>")

 14:00~17:30 ◇ 장 소 : 건강보험심사평가원 본원 지하대강당 ◇ 주 관 : 건강보험심사평가원.>")



 로 인하여 후쿠시마 제 1 원자력발전소에서 발생한 사고. 발전소가 침수되어 전원 및 냉각 시스템이 파손되면서 핵연료 용융과.>")




 비만률순위 : 29 위 (2005 OECD)>")





