Download presentation
1
Video Conference R3 임성아/Ap. 김규섭

2
Chief Complaint 52/M Dec.VA (OS) onset : 1m ago 시력저하 소견 잘 모르다가 우연히 좌안
시력저하되었음을 인지 VA OD 0.8 OS (n-c)
")
3
Past histoty DM/ HBP(-/-) Brain tumor (+)
Diffuse large B cell Lymphoma frontal Lt. s/p craniotomy c tumor removal s/p MTX CTx c RTx. Ocular op/ Trauma (-/-) Gls (-) Eyedrop (-) (diffuse large B-cell type) MRI no new lesion NS -MRI f/u no newly developed enhancing lesion known CNS lymphoma since April
 Gls (-) Eyedrop (-) (diffuse large B-cell type) MRI no new lesion. NS -MRI f/u no newly developed enhancing lesion. known CNS lymphoma since April")
4
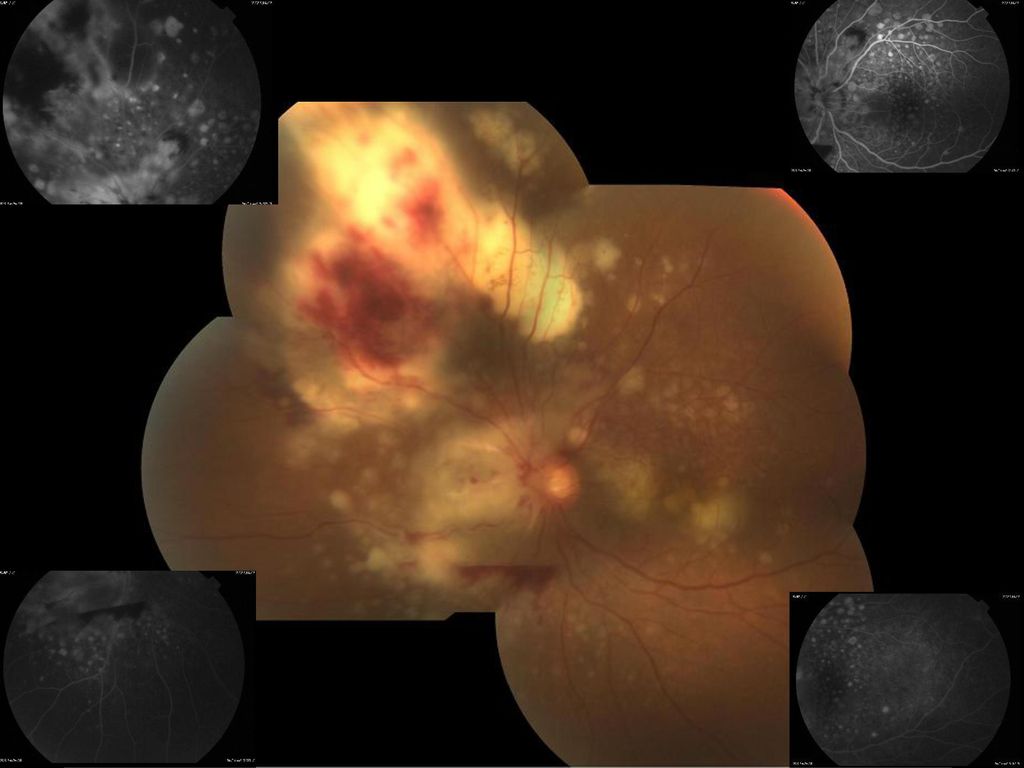
Physical examination MR OD +0.50Ds=-0.50Dc Ax 60 OS +1.00Ds=-1.00Dc Ax 105 IOP 15/14 mmHg Lid no swelling Conj. not injected Cornea clear AC deep & cell(trace) Pupil round & nl. sized ( LR +) RAPD (-/+-) Lens clear / (OU) FD OD : CDR 0.7/0.7 c flat post.pole OS : Disc swelling c multiple subretinal yellow lesion c pre-retinal & retinal lesion R/O vasculitis OS R/O CMV retinitis OS uveitis lab환자분 사정상 당일 입원 어려움.수요일 adm (FAG(imagenet으로), HRA oS->OD, SD OCT HD5 V&H os, mosaic photo os)당일 신경외과 consult for brain evaluation diagnostic ppV 5/20
6
Differential diagnosis
Lymphoma Male Unilateral R/O Intraocular lymphoma R/O Vsculitis R/O CMV retinitis Plan ) Ocular lab : B-scan, FAG , OCT Uveitic lab 3. NS consultation for brain evaluation 4. Diagnostic ppV schedule
 Ocular lab : B-scan, FAG , OCT. Uveitic lab. 3. NS consultation for brain evaluation. 4. Diagnostic ppV schedule.")
7
2011.5.20 Diagnostic ppV +intravit. MTX inj. (OS)
8
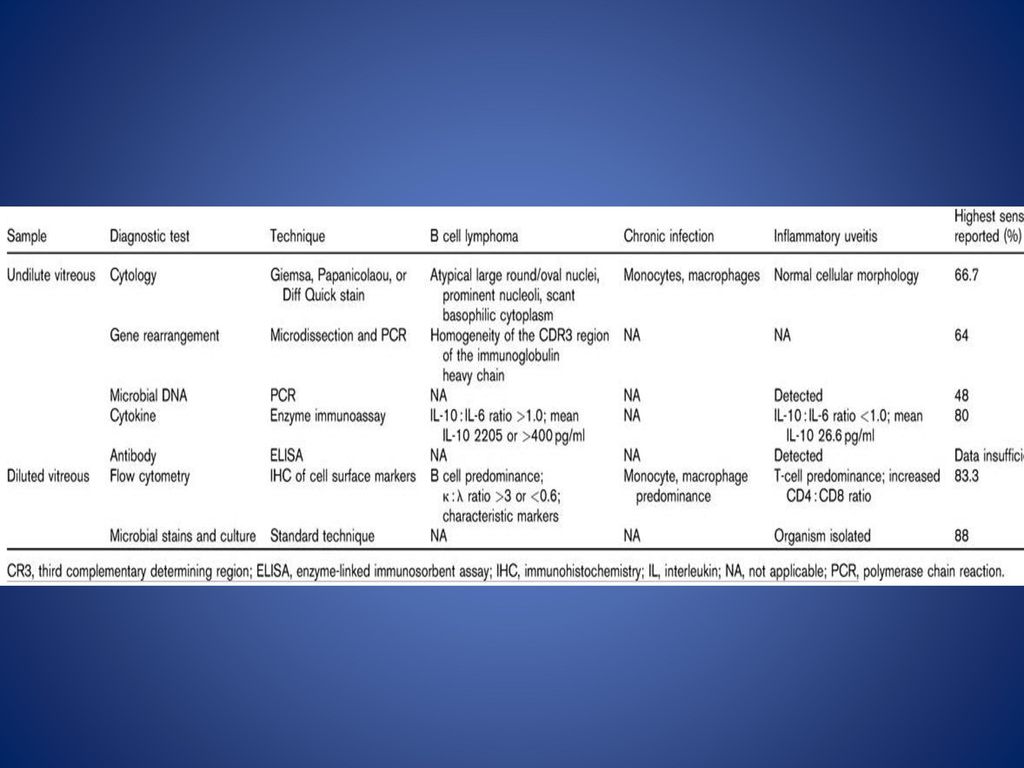
Diagnostic test sample Culture Gram stain Fungal culture (-) Cytopathology Atypical cells suspicious of Malignant lymphoma involvement. PCR M. Tuberculosis (PCR & Hybrid) Toxoplasma DNA PCR VZV CMV RQ –PCR HSV type 1PCR Flow cytometry IGH/ IGK/ IGL Mono- clonality assays (+/+/+)
 Toxoplasma DNA PCR. VZV. CMV RQ –PCR. HSV type 1PCR. Flow cytometry. IGH/ IGK/ IGL. Mono- clonality assays. (+/+/+)")
9
Cytopathology /Monoclonal assays

10
Non-Hodgkin lymphoma (Primary CNS lymphoma)
OS (VA) 1 2 (0.16) 3 4 (0.5) 5 6 (0.5) 7 (0.4) 8 (0.4) 9 (0.16) ~ 9 th Intravitreal MTX inj. (OS) Hematology adm. MTX 3.5g/m2 + ARA 2g/m2 bid
 (0.16) (0.5) (0.5) (0.4) (0.4) (0.16) ~ th Intravitreal MTX inj. (OS) Hematology adm MTX 3.5g/m2 + ARA 2g/m2 bid.")
12
Chief Complaint 25/F Dec.VA (OD) onset : 1wks ago
VA OD 0.02(0.06 x -3.75Ds) – 윗쪽으로 OS 0.2 (1.0 x -4.25Ds)
 – 윗쪽으로. OS 0.2 (1.0 x -4.25Ds)")
13
Past histoty DM/ HBP(-/-) Ocular op/ Trauma (-/-) Gls (-)
Eyedrop (+) O-LON x q2hrs(OD) PO (+) Bactrim 1T#2 Albendazole 800mg #2 * 국립중앙의료원 방문 : 우안 망막 이상으로 uveitic lab진행 * 동생이 TB medi. 중 상기 25세 여자 환자는 부터 시작된 우안의 중심시력저하를 주소로 에 국립중앙의료원 방문하여 정방과 유리체에 염증세포가 관찰되지 않았으나 황반 중심에서 비측으로(juxtafovea) 1/2 DD sized retinal opacification 보여 형광안저 촬영 및 OCT 촬영하였고, toxoplasmosis 의심되어 lab 시행하였음. 에 두번째 내원시 AC cell(3+), Vit. cell(1+) 소견 보이고 retinal opacitication이 중심와 중심 쪽으로 진행하였으며, 시력도 더 저하되었음. 에 toxocara에 관련된 검사실 검사 처방했고, Bactrim 2T bid, 알벤다졸 800mg bid, O-LON x q2hrs(OD) 처방하였고, 본원 진료 원하여 본과 내원함. 전신질환(-) toxoplasma Ig M/G(-/-) syphilis (-) HIV (-) Hepatitis B carrier chest n-s
 O-LON x q2hrs(OD) PO (+) Bactrim 1T#2. Albendazole 800mg #2. * 국립중앙의료원 방문 : 우안 망막 이상으로 uveitic lab진행. * 동생이 TB medi. 중. 상기 25세 여자 환자는 부터 시작된 우안의 중심시력저하를 주소로 에 국립중앙의료원 방문하여 정방과 유리체에 염증세포가 관찰되지 않았으나. 황반 중심에서 비측으로(juxtafovea) 1/2 DD sized retinal opacification 보여. 형광안저 촬영 및 OCT 촬영하였고, toxoplasmosis 의심되어 lab 시행하였음 에 두번째 내원시 AC cell(3+), Vit. cell(1+) 소견 보이고. retinal opacitication이 중심와 중심 쪽으로 진행하였으며, 시력도 더 저하되었음 에 toxocara에 관련된 검사실 검사 처방했고, Bactrim 2T bid, 알벤다졸 800mg bid, O-LON x q2hrs(OD) 처방하였고, 본원 진료 원하여 본과 내원함. 전신질환(-) toxoplasma Ig M/G(-/-) syphilis (-) HIV (-) Hepatitis B carrier. chest n-s.")
14
Physical examination MR OD +0.50Ds=-0.50Dc Ax 60 OS +1.00Ds=-1.00Dc Ax 105 IOP 15/19 mmHg Lid no swelling Conj. not injected Cornea clear Pupil round & nl. sized ( LR +) RAPD (-/+-) Lens clear / (OU) AC OD deep & cell(+) OS deep & cell(-) FD OD blurry disc margin c whitish retinal lesion at macula, vit. Cell(+) OS nl. Optic disc c flat post pole
15
FAG(OD) FAG & ICG (OD) 3.85sec 15 sec 7 분
 FAG & ICG (OD) 3.85sec 15 sec 7 분")
16
Differential diagnosis
Panuveitis(OD) Retinitis (OD) R/O Toxoplasma R/O Toxocariosis R/O Candida Plan ) Uveitic lab Chest CT PO & eyedrop Toxoplasma Ig M/G(-/-) DNA PCR (-) Toxocariosis Ig G (-) Candida Ag/ Ab (-/+) Ig E (inc. ) Chest CT – n-s
 Retinitis (OD) R/O Toxoplasma. R/O Toxocariosis. R/O Candida. Plan ) Uveitic lab. Chest CT. PO & eyedrop. Toxoplasma Ig M/G(-/-) DNA PCR (-) Toxocariosis Ig G (-) Candida Ag/ Ab (-/+) Ig E (inc. ) Chest CT – n-s.")
17
PO VA 2011.12.19 1st. visit Albendazole Bactrim 0.02 (0.06) 2011.12.22
A+B Add H-LON 30mg x7d (0.04) H-LON 20mg x7d (0.02) B+H-LON 5mg add Fluconazole 1T add praziquantel 3T (0.125 ) Fluconazole 1T praziquantel 3T Restart A (0.1) A+ H-LON 30mg (0.06) Diagnostic ppV (OD) stationary cell(trace ) 로 감소 / whitish retinal lesion 감소 cell (rare) vit. Cell (+) inc. Fd whitish retinal lesion at macula od : progression? iop14/14AC cell (rare) vit cell (+) increased , opacity Fd whitish retinal lesion at macula, od : progression new Hm
18
2012.1.27 Diagnostic ppV +Intravit amphotericin B inj.(OD)
")
19
Negative for malignancy (-/-/-) Flow cytometry
Diagnostic test sample Culture KOH Gram stain Fungal culture (-) (+) Candida albicans Biopsy Cytology Gomori/ Silver/ PAS Negative for malignancy (-/-/-) Flow cytometry M. Tuberculosis (PCR & Hybrid) Toxoplasma DNA PCR VZV CMV RQ –PCR HSV type 1PCR Aspergillic Ag 0.10 (<0.5) Vitreou(D), Cassette) Answer key: 1D, 2B, 3B, 4C, 5B, 6A, 7D, 8A, 9B, 10D
 (+) Candida albicans. Biopsy. Cytology. Gomori/ Silver/ PAS. Negative for malignancy. (-/-/-) Flow cytometry. M. Tuberculosis (PCR & Hybrid) Toxoplasma DNA PCR. VZV. CMV RQ –PCR. HSV type 1PCR. Aspergillic Ag (<0.5) Vitreou(D), Cassette) Answer key: 1D, 2B, 3B, 4C, 5B, 6A, 7D, 8A, 9B, 10D.")
20
Retinal candidiasis 다시 history 1년전 질염으로 약먹고 치료 현재는 괜찮음.
다이어트 주사 10회 피하주사 맞음 (배 , 허벅지) 카복시, 메조테라피 Tx. ) Eyedrop (+) O-GAFx4, O-LONxq2h, O-1AT x2 (OD) PO fluconazole 150mg Consultation for OBGY, MI
 카복시, 메조테라피. Tx. ) Eyedrop (+) O-GAFx4, O-LONxq2h, O-1AT x2 (OD) PO fluconazole 150mg. Consultation for OBGY, MI.")
21
POD #1d POD #12d iop 8/14c/c 2일전 부터 통증 AC cell (+) lens mild PSC
vit cell (++) Fd dec multiple whitish retinal or preretinal lesion dec whitish retinal lesion at macula vascular sheathing (-) 2.25 일부터 나빠짐 POD #12d
22
Chief Complaint 54/F Dec.VA (OD) onset : 골수이식후
ALL로 월 골수 이식 받고, 9월에 퇴원 후 지속적으로 우안 시력 저하 소견 1주일 전부터 우안 시력저하 심화되어 내원 VA OD fC 50cm ( n-c) OS 0.8 내원
 OS 내원.")
23
Physical examination MR OD error OS -1.00Ds=-1.00Dc Ax 95 IOP 15/16 mmHg Lid no swelling Conj. not injected Cornea clear Pupil round & nl. sized Lens clear / (OU) AC OD deep & cell(++++) c iris pigment (+) OS deep & cell (-) Fds OD blurry d/t vit opaicity, suspicious retinal hm at parafovea c diffuse whitish retinal necrotic lesion OS nl. optic disc c flat post.pole F-photo(OU) adm recommend MH consult O-GAF x4 O-1AT x 2/OD 1인실 병식 밖에 없는 상태이며, 격리실은 ANC 500이상으로 해당이 안되어 우선 귀가 후 내일 외래 f/u 하면서 입원하시기로 설명드림. /R2박창현/Ap.김규섭
24
CMV retinitis(OD) 2011.11.22, AC paracentesis(OD) CMV PCR (+)
Intravitreal Ganciclovir inj. (OD) 0.02 FC 50cm FC 30cm Intravitreal foscarnet inj. (OD) FC 50cm
25
12.1.11 ppV+ppL +intravit. ganciclovir inj.(OD)
27
Review Diagnostic ppV R3 임성아/Ap. 김규섭

28
Vitreous humor anatomy
Gel like - long non branching collagen fibrils - glycosaminoglycan chains Variable attachment Vitreous loss lead to complication

29
Vitrectomy Therapeutic ppV: VITRECTOM V-vitreous Hm. I –infection
Diagnostic ppV: Infection malignanacy Therapeutic ppV: VITRECTOM V-vitreous Hm. I –infection T-traction R-retinal detachment E-epiretinal Membrane C-cataract related complication T-trauma O-opacity of vitreous cavitiy M-macular disease

30
Vitreous biopsy Vitreous aspiration - simple - risk for VRT, RD
Diagnostic ppV Large amount of sample Removing most of the pathologic material from the eye 3. Better diffusion of intraocular medications 4. Post operative fundus exam - clear

31
Starting vitrectomy Know your step Microscope –footswitch
Vitrectomy footswitch Infusion Vitrectomy probe Light source Lens – contact / noncontacct

32
1.vitreous specimen is collected through undiluted lines using the vitreous cutter connected directly to a syringe ( until the eye is noted to soften visibly) 2.Dilute vitreous from the second syringe & Vitrector cassette The vitreous specimen is collected through undiluted lines using the vitreous cutter connected directly to a 3-ml syringe until the eye is noted to soften visibly (Fig. 1). In our experience, at least 1.5 ml of undiluted vitreous can be reliably obtained using this technique. The infusion is then started, and diluted vitreous is aspirated into a second syringe. The amount of vitreous obtained is limited by complication of hypotony such as suprachoroidal hemorrhage; therefore, Quiroz-Mercado et al. [2] described perfluorocarbon-perfused vitrectomy
34
<Cytopathology> ‘gold standard’ diagnosis of malignancy ‘
< Flow cytometry> analysis of different cell surface markers demonstration of monoclonality (CD22 , CD20, [kappa] ,[lambda] chain ) < Molecular analysis & PCR> Gene arrangement , DNA < Microbiological stain & culture> Gram stain Fungal & bacterial cultrue
 < Molecular analysis & PCR> Gene arrangement , DNA. < Microbiological stain & culture> Gram stain. Fungal & bacterial cultrue.")
35
Thank you for your attention !











 recent 2wks ago remote 10yrs ago Present Illness 72/M, HTN, angina 로 본원 IC(Pf. 김우식 ), DM 으로 본원 IE(Pf. 오승준 ) f/u 하는.>")
 Adm 2012.03.28 주소 Cough onset time) 내원 1 달 전 현병력 60 세 여자환자. HTN, dyslipidemia 로 타 병원에서 medication.>")








