Download presentation
Presentation is loading. Please wait.

1
Young-Hee Sung, M.D. Department of Neurology Asan Medical Center
쓸모없는 왼손을 가진 63세 여자환자 Young-Hee Sung, M.D. Department of Neurology Asan Medical Center

2
Clinical History C/C Useless left hand since 6 months ago
P/I 세 여자환자는 별다른 medical problem 없이 지내오던 분으로 03년 10월에 두통으로 W 병원 방문하여 Brain MRI 찍고 뇌경색 소견과 고혈압 있어 침과 한약, 양약을 같이 투약 04년 5월에는 예전처럼 농사일을 하면서 오른손 으로 호미질하고 왼손으로 씨를 심었음.

3
Clinical History P/I 04년 8월 고추를 따서 말리는데 왼손이 말을 듣지
않아 모든 일을 오른손으로 하여서 당시 아들이 G 한방병원에서 한약을 지어와서 2달간 먹었으나 증상은 호전이 없었고 진행됨 04년 12월 왼팔이 뻣뻣하게 굳어 펴지지 않아 W병원 신경과 내원하여 Parkinsonism 진단하에 medication 시작 05년 2월에 걸음이 쏟아지듯 걸어져서 5차례 넘어져 further manage 위해 본원 외래 방문함

4
Clinical History PMHx DM/HTN/Tbc/Hepa (-/+/-/-) FHx Unremarkable
OP/Adm(-/-) 03년 HTN, Silent infarction 로 medication start 04년 12월 Parkinsonism 로 medication start FHx Unremarkable
 03년 HTN, Silent infarction. 로 medication start. 04년 12월 Parkinsonism 로. medication start. FHx Unremarkable.")
5
Clinical History SHx 초졸 ROS Postural dizziness (-) 농부 Smoking (-)
Voiding difficulty (+) ; frequency 1-2hr nocturia #2/night Constipation (-) Vivid dream (-) Abnormal behavior during sleep (-) Hallucination (-)
 ; frequency 1-2hr. nocturia #2/night. Constipation (-) Vivid dream (-) Abnormal behavior during sleep (-) Hallucination (-)")
6
Clinical History Physical Examination V/S 134/72-77-22-36.0℃
G/A Relative good looking appearance HEENT Anicteric sclera Chest Normal breath and heart sound Abd. No organomegaly Ext No cyanosis or skin lesions

7
Clinical History Neurologic Examination HCF MMSE 27/30
M/S Alert HCF MMSE 27/30 Frontal lobe releasing sign Glabella reflex (+) Snout (+) Palmomental reflex (-) Grasping reflex(-) Ideomotor apraxia (+) ; bilateral(Lt>Rt) BPO error Ideational apraxia (-) Cortical sensory Ex Two point discrimination ; Rt – 11mm Lt -12mm Graphesthesia (+) ; Rt - 4/10, Lt - 2/10 Astereognosis (-) Sensory extinction (-) Anosognosia (-) Asomatognosia(-)
 Snout (+) Palmomental reflex (-) Grasping reflex(-) Ideomotor apraxia (+) ; bilateral(Lt>Rt) BPO error. Ideational apraxia (-) Cortical sensory Ex. Two point discrimination ; Rt – 11mm Lt -12mm. Graphesthesia (+) ; Rt - 4/10, Lt - 2/10. Astereognosis (-) Sensory extinction (-) Anosognosia (-) Asomatognosia(-)")
8
Clinical History Neurologic Examination
CNF Isocoric pupil with PLR (++/++) EOM - full without nystagmus VF - intact Motor All Gr. V Sensory Intact DTR Normoactive without pathologic reflex
 EOM - full without nystagmus. VF - intact. Motor All Gr. V. Sensory Intact. DTR Normoactive without pathologic reflex.")
9
Clinical History Neurologic Examination
Speech & Facial expression : OK Tremor at rest /0 Rigidity axial 0 U/Ex 0/ 3 L/Ex 0/2 Bradykinesia U/Ex 1/2 L/Ex 0/1 Postural instability 0 Gait Lt arm swing 감소

10
VIDEO Presentation

12
Clinical Summary Lt arm dystonia & rigidity Ideomotor apraxia
Cortical sensory impairment Frontal lobe dysfunction

13
Clinical Diagnosis Corticobasal Ganglionic Degeneration

14
Neuropsychological Test

15
Neuropsychological Test - SNSB
K-MMSE 27/30 Attention Digit span, Forward / Backward 4/0 Language Spontaneous speech, comprehension, repetition Normal Korean Boston Naming Test 25/60(0.13%ile) Reading, Writing, Finger naming Praxis Abnormal Body part identification, Rt.-Lt. Orientation, Calculation Visuospatial function Interlocking pentagon Rey CFT copy 30/36(27.09 %ile) Memory Orientation, Time / Place 5 / 4 3 words, registration / recall 3 /3 Remote memory 6 MMSE에서 place orinetation에서 1점, serial seven에서 2점 감점되어 27점 Digit span에서 forward 4, backward 0점으로 주의집중능력 및 working memory 의 저하가 관찰되었음 언어 기능에서는 confrontational naming ability 의 저하가 관찰됨 Praxis 검사중 휘파람 부는 흉내에서 흉내를 내지 못하고 ‘훼,훼’ 라고 소리만 내는 오류를 보이는 경미한 Buccofacial apraxia가 관찰됨, 또한 ideomotor apraxia검사에서 모든 항목에서 BPO error가 양손에서 관찰됨 시공간 기능은 잘 유지되고 있었으며, micrographia가 관찰됨 언어적 기억력은 잘 유지가 되고 있음
 Reading, Writing, Finger naming. Praxis. Abnormal. Body part identification, Rt.-Lt. Orientation, Calculation. Visuospatial. function. Interlocking pentagon. Rey CFT copy. 30/36(27.09 %ile) Memory. Orientation, Time / Place. 5 / 4. 3 words, registration / recall. 3 /3. Remote memory. 6. MMSE에서 place orinetation에서 1점, serial seven에서 2점 감점되어 27점. Digit span에서 forward 4, backward 0점으로 주의집중능력 및 working memory 의 저하가 관찰되었음. 언어 기능에서는 confrontational naming ability 의 저하가 관찰됨. Praxis 검사중 휘파람 부는 흉내에서 흉내를 내지 못하고 ‘훼,훼’ 라고 소리만 내는 오류를 보이는 경미한. Buccofacial apraxia가 관찰됨, 또한 ideomotor apraxia검사에서 모든 항목에서 BPO error가 양손에서 관찰됨. 시공간 기능은 잘 유지되고 있었으며, micrographia가 관찰됨. 언어적 기억력은 잘 유지가 되고 있음.")
16
Neuropsychological Test -SNSB
Memory SVLT, Free recall 1st / 2nd / 3rd // delayed recall Recognition: true positive-false positive 4/5/9//6 10-1(43.25%ile) Rey CFT copy/ immediate recall/ delayed recall 7.5(14.46%ile)/ 7.5(6.55%ile) 11-3(82.38%ile) Frontal/ Executive Function Contrast program Normal Fist-edge-palm / Alternating hand movement / Go-No-Go test Abnormal Alternating square-triangle / Luria loop Deformed Perseveration COWAT, 동물/ 가게물건 //ㄱ / ㅇ / ㅅ 13/ 11//1/0/0 Stroop test(글자읽기/색깔 읽기) 88/0 // 28/0 시각적 기억검사에서 즉각회사과 지연회상에서 수행의 저하가 관찰되었으나 재인에서 수행의 향상이 관찰되므로 정보의 인출에 어려움을 보이는 시각적 기억장애로 판단됨 Contrast program, Go-No-G0 test에서 대부분 검사자의 행동을 그래로 따라한후 교정하는 양상을 보이고 Go-No-Go test 에서 부분적으로 이전규칙을 적용하는 오류를 보이는 양상의 Mental set shifting에 어려움이 관찰됨 Fist-edge-palm, alernating square-triangle에서 motor set shifting에 어려움이 관찰됨 Alternating square-triangle 에서 그림이 deform되어 반복되는 양상을 보였고 Luria loop에서 perseveration관찰됨 Word fluency의 저하가 관찰 Stroop test에서 글자읽기에 비해서 색깔읽기 수행의 저하가 관찰되므로 이는 inhibitory control ability저하가 있는것으로 판단
 Rey CFT copy/ immediate recall/ delayed recall. 7.5(14.46%ile)/ 7.5(6.55%ile) 11-3(82.38%ile) Frontal/ Executive. Function. Contrast program. Normal. Fist-edge-palm / Alternating hand movement / Go-No-Go test. Abnormal. Alternating square-triangle / Luria loop. Deformed. Perseveration. COWAT, 동물/ 가게물건 //ㄱ / ㅇ / ㅅ. 13/ 11//1/0/0. Stroop test(글자읽기/색깔 읽기) 88/0 // 28/0. 시각적 기억검사에서 즉각회사과 지연회상에서 수행의 저하가 관찰되었으나. 재인에서 수행의 향상이 관찰되므로 정보의 인출에 어려움을 보이는 시각적 기억장애로 판단됨. Contrast program, Go-No-G0 test에서 대부분 검사자의 행동을 그래로 따라한후 교정하는 양상을 보이고. Go-No-Go test 에서 부분적으로 이전규칙을 적용하는 오류를 보이는 양상의 Mental set shifting에 어려움이 관찰됨. Fist-edge-palm, alernating square-triangle에서 motor set shifting에 어려움이 관찰됨. Alternating square-triangle 에서 그림이 deform되어 반복되는 양상을 보였고 Luria loop에서 perseveration관찰됨. Word fluency의 저하가 관찰. Stroop test에서 글자읽기에 비해서 색깔읽기 수행의 저하가 관찰되므로 이는 inhibitory control ability저하가 있는것으로 판단.")
17
Neuropsychological Test -SNSB
Alternating square-triangle Luria loop

18
Neuropsychological Test -SNSB
전두엽 집행기능의 저하가 주로 관찰

19
Neuropsychological Test -SNSB
인출에 어려움을 보이는 시각적 기억장애

20
Neuropsychological Test
Spatial neglect Line bisection ; 6mm midline에서 Rt로 치우침 Star cancellation ; Lt side 4개 빠뜨림 Ogden picture, two Daisy 보고 그리기 : OK Praxis 상지 구두명령 ; Rt – 15/15, Lt – 15/15 얼굴 구두명령 ; 14/15 도구사용 구두명령 ; Rt -11/15, Lt -5/15 도구 사용 실물사용 ; Rt -15/15, Lt – 12/15 판토마임 재인검사 ; 20/30

21
Neuropsychological Test
Line bisection Star cancellation

22
Neuropsychological Test Summary
Both frontal lobe dysfunction Ideomotor apraxia Mild buccofacial apraxia Hemineglect

23
Brain Imaging

24
Brain MRI 03년 10월 22일 - 외부 필름 Chronic ischemic change of both periventricular white matter. Old infarct, right BG and corona radiata. No acute diffusion abnormality. Intact intracranial vessels and carotid bifurcations.

25
Brain MRA 03년 10월 22일 - 외부 필름

26
Brain MRI 05년 3월 8일 검사상 양쪽 periventricular white matter에 chronic ischemia와 right basal ganglia와 corona radiata쪽의 infarction을 의심했던 환자임. 그러나 follow-up에서도 비슷한 정도의 T2 signal change를 보이고 있고 infarction으로 interpretation한 부분의 T1 WI에서의 signal의 양상을 볼때 overt한 infarction 보다는 역시 ischemic change에 의한 signal change로 생각됨. Abnormal enhancement 없음. No interval change of chronic ischemic change involving both periventricular white matter and basal ganglia. No overt infarction.

28
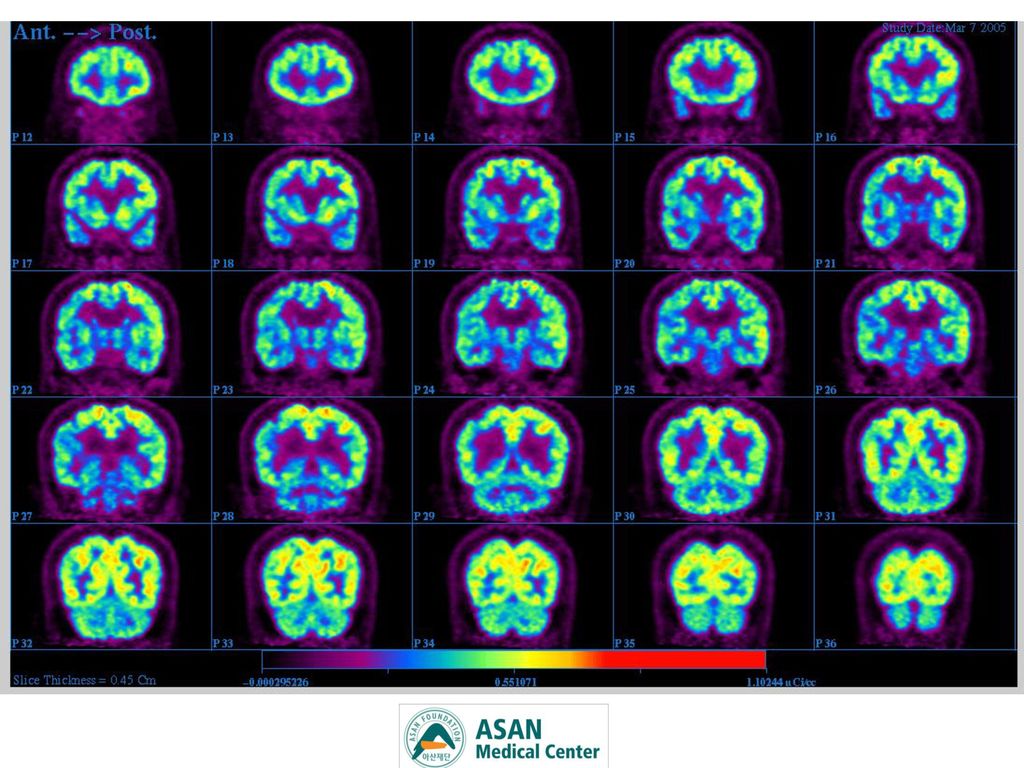
Right fronto-parietal cortex와 right basal ganglia, thalamus, right side of mid brain의 metabolism이 left side에 비해 slightly decreased되어 있음. Slightly decreased metabolism of right basal ganglia, thalamus, basal ganglia and fronto-parietal cortex

29
SPM2를 이용하여 같은 연령의 11명 정상인과 T-test한 결과로 theshold는 P<0
SPM2를 이용하여 같은 연령의 11명 정상인과 T-test한 결과로 theshold는 P<0.01, extent theshod >100 voxel에서 정상인에 비해 유의하게 metabolism이 감소한 부위를 MNI template에 display한 surface render and 3D sectional image입니다.

30
? CBD vs ? Vascular Parkinsonism

31
Vascular lesion ? 05년 3월 8일 03년 10월 22일

32
Vascular lesion ? 03년 10월 22일 05년 3월 8일

33
Cortical lesion? 03년 10월 22일 05년 3월 8일

34
Cortical lesion? 03년 10월 22일 05년 3월 8일

35
? CBD vs ? VP Sx (-) B-MRI = Sx(+) B-MRI Threshold effect ??
IPD 환자에서 substantia nigra의 세포가 50-70%가 이미 죽은 상태이며 striatum 의 dopamine이 80%정도 고갈되었을때 임상증상이 나타난다. Threshold effect ??

36
? CBD vs ? VP Progressive course Upper extremity rigidity Cortical Sx
Ideomotor apraxia Cortical sensory impair Hemineglect Rt parietal cortex atrophy HTN Hx Multiple Basal ganglia & subcortical launar lesion

37
Final Diagnosis Vascular CBD

38
CASE REVIEW Overview of CBD Relationship between FTD and CBD
Vascular CBD Apraxia in CBD

39
Review Overview of CBD

40
History Arch Neurol 1968; 18: 20–33
Rebeiz and colleagues Three patients with slow and awkward voluntary limb movement, tremor, dystonic posturing, stiffness, lack of dexterity, “numbness or deadness” of the affected limb, and gait disorder. Identified by asymmetrical frontoparietal cortical atrophy and neuronal loss, associated gliosis, and swelling of the neuronal cell bodies, which were devoid of Nissl substance (hence the term achromasia). “corticodentatonigral degeneration with neuronal achromasia”
. corticodentatonigral degeneration. with neuronal achromasia")
41
Epidemiology Lancet Neurol 2004; 3: 736-43
Onset of symptoms ; sixth to eighth decades mean age ; 63 years (SD 7·7) Sporadic disease, rare familial cases Togasaki and Tanner estimated that corticobasal degeneration accounts for 4–6% of parkinsonism, and according to the incidence of Parkinsonism the incidence of corticobasal degeneration would be 0.62–0.92 per per year Mean survival ; 7.9 years
 Sporadic disease, rare familial cases. Togasaki and Tanner estimated that corticobasal. degeneration accounts for 4–6% of parkinsonism, and according to the incidence of Parkinsonism. the incidence of corticobasal degeneration would be. 0.62–0.92 per per year. Mean survival ; 7.9 years.")
42
Proposed Criteria for the Diagnosis
Insidious onset and progressive course No identifiable cause (eg, tumor, infarct) Cortical dysfunction Focal or asymmetrical ideomotor apraxia Alien Limb phenomenon Cortical sensory loss Visual or sensory hemineglect Constructional apraxia Focal or asymmetric myoclonus Apraxia of speech/nonfluent aphasia Extrapyramidal dysfunction Focal or asymmetrical appendicular rigidity lacking prominent and sustained L-dopa response Focal or asymmetrical appendicular dystonia Core Feature
 Cortical dysfunction. Focal or asymmetrical ideomotor apraxia. Alien Limb phenomenon. Cortical sensory loss. Visual or sensory hemineglect. Constructional apraxia. Focal or asymmetric myoclonus. Apraxia of speech/nonfluent aphasia. Extrapyramidal dysfunction. Focal or asymmetrical appendicular rigidity lacking prominent and sustained L-dopa response. Focal or asymmetrical appendicular dystonia. Core Feature.")
43
Proposed Criteria for the Diagnosis
Supportive Feature Variable degrees of focal or lateralized cognitive dysfunction, with relative preservation of learning and memory, on neuropsychological testing Focal or asymmetric atrophy on CT or MRI, typically maximal in parietofrontal cortex Focal or asymmetric hypoperfusion on SPECT or PET, typically maximal in parietofrontal cortex ± basal ganglia ± thalamus

44
Review 2. Relationship between FTD and CBD

45
Classification of FTD Pathologic variants FTLD-ldh FTLD-Pick(Pick dis)
MND Clinical variants Frontotemporal dementia FTDP-l Progressive aphasia FTD-MND Corticobasal degneration FTLD-l dh : dementia lacking distinctive histology Pick cell : typical ballooned neuron FTE-MND : tau-negative inclusions of the motor neuron disease type Primary progressive aphasia Progressive nonfluent aphasia Progressive language disorder Semantic dementia Progressive fluent aphasia Temporal variant of FTD

46
Neuropathological Overlap
Relationship between FTD and CBD Dement Geriatr Cogn Disord 2004;17:282–286 Neuropathological Overlap Presence of focal atrophy and ballooned neurons The cytoplasmic inclusions in CBD cortical neurons often adopt a rounded morphology, and thus are indistinguishable from Pick bodies on Bielchowsky stains, or for that matter most tau immunostains. Astrocytic argyrophilic inclusions that bind tau antibodies The oligodendroglia is affected

47
Relationship between FTD and CBD Dement Geriatr Cogn Disord 2004;17:282–286
Cognitive and Behavioral Change in CBD 35 patients with clinical CBDS 21 patients (60%) developed all three syndromes of movement disorder, language decline, and behavioral symptoms. In 11 of our 35 cases with autopsy, 6 had CBD pathology, 3 cases had PiD,1 had MND-type inclusions, and 1 superficial spongiosis, gliosis, and neuronal loss, also called DLDH. Frontal lobe dysfunction with behavioral disturbances is described in at least 50% of the patients with CBD
 developed all three syndromes. of movement disorder, language decline, and. behavioral symptoms. In 11 of our 35 cases with autopsy, 6 had CBD. pathology, 3 cases had PiD,1 had MND-type inclusions, and 1 superficial spongiosis, gliosis, and neuronal. loss, also called DLDH. Frontal lobe dysfunction with behavioral disturbances. is described in at least 50% of the patients with CBD.")
48
Relationship between FTD and CBD Dement Geriatr Cogn Disord 2004;17:282–286
The Genetic Overlap Chromosome 17-linked familial FTD and parkinsonism closely resembles the syndromes of Pick complex, and the atypical parkinsonism is similar to CBD and PSP

49
Review Vascular CBD

50
Vascular Parkinsonism J Neurol (2004) 251 : 513–524
Not only can vascular lesions rarely masquerade as IPD, but they can also cause some clinical features of other primary degenerative diseases causing parkinsonism such as PSP, MSA and CBD A subtype of PSP due to vascular causes (“vascular PSP”) has been proposed.
 has been proposed.")
51
Vascular PSP J Neural Transm Suppl. 1994;42:189-201.
128 patients diagnosed with PSP 23.3% of PSP cases satisfied criteria for vascular PSP. The vascular group differed from the idiopathic group by asymmetric and predominantly lower body involvement . (p < 0.05) Corticospinal signs, pseudobulbar signs, gait difficulties, dementia, and incontinence of bowels and bladder were also more common in the vascular group, but these differences did not reach statistical significance.
 Corticospinal signs, pseudobulbar signs, gait difficulties, dementia, and incontinence of bowels and bladder were also. more common in the vascular group, but these differences did not reach statistical significance.")
52
Vascular Parkinsonism J Neurol (2004) 251 : 513–524
Cases combining basal ganglia and parietal infarcts or supplementary motor area(SMA) alone may mimic some of the clinical features of CBD: limb apraxia, limb dystonic posturing, motor slowness and sensory deficits. These cases are however rare and simply diagnosed by neuroimaging
 alone may mimic some of the. clinical features of CBD: limb. apraxia, limb dystonic posturing, motor slowness and sensory. deficits. These cases are however rare. and simply diagnosed by. neuroimaging.")
53
Review Apraxia in CBD

54
Apraxia in CBD Apraxia - a hallmark of CBD and is an important component of all proposed diagnostic criteria Of equal importance, it is a source of misdiagnosis: Patients with parkinsonism plus apraxia are typically diagnosed as having CBD rather than the more appropriate designation of ‘cortical-basal syndrome’ (CBS) CBS may be caused by a variety of underlying CNS pathologies, including PSP, AD, DLB and FTD
 CBS may be caused by a variety of underlying CNS pathologies, including PSP, AD, DLB and FTD.")
55
Apraxia in CBD Ideomotor limb apraxia In ‘classic’ CBD
2 types of apraxias : ideomotor and limb-kinetic Ideational apraxia : a late feature related to more severe dementia Ideomotor limb apraxia most commonly recognized type of apraxia commonly bilateral but typically asymmetrical, especially early in the disease course consist of spatial, temporal and sequencing errors more frequently when performing transitive than intransitive tasks often improve when the subject is given an object to use

56
Apraxia in CBD Visuokinaesthetic motor engrams ‘praxicon’
: stored in the Parietal lobe SMA Pimary motor cortex In the anterior type of IMA damage to the SMA or to subcortical white matter which disconnects motor areas from the intact parietal lobe patients can recognize gestures easily however, the information on how to perform the gesture is lost Pathological involvement in classical CBD - superior frontal, precentral, postcentral gyri

57
Apraxia in CBD Limb-kinetic apraxia (LKA)
consists of impaired, coarse, ‘mutilated’ execution of simple movements of the hand contralateral to the cortical lesion most notable for incoordination between fingers, as seen in object manipulation tasks and fine finger movements usually unilateral IMA : typically bilateral more evident distally than proximally difficult to distinguish from bradykinesia, rigidity and dystonia

58
Apraxia in CBD Leiguarda et al. (2003)
clinical and kinematic features of LKA 5 CBD / 5 PD /10 controls All 5 CBD patients - a unilateral praxic deficit characterized by chaotic movement with marked interfinger incoordination neurological abnormalities such as bradykinesia and rigidity alone are not able to explain LKA dysfunction in the premotor cortex accounts for LKA Finally, clinicopathological evidence in 5 patients also supports the role of damage to the premotor cortex underlying LKA in CBD

59
Thank You For Your Attention

Similar presentations



















 Brain CT 건국대학교 충주병원 영상의학과>")
