Download presentation
Presentation is loading. Please wait.

1
Nonoperative management of incontinence Hyun Un Cho. MD
Nonoperative management of incontinence Hyun Un Cho. MD., Hwamyeong Jangsiwon Hospital

2
Factor should consider to treat Incontinence
1.Anal sphincter function and pelvic floor function 2. Anal sphincter morphology 3. Pudendal nerve function 4. Rectal reservoir function (sensation, compliance, capacity) 5. Rectal evacuation Gastrointestinal (primary colonic) transit
 5. Rectal evacuation Gastrointestinal (primary colonic) transit.")
3
Factor associated with increasing Symptom Severity of Incontinence Abnormal colonic motility Obesity Pelvic floor disorder History of episiotomy

4
Factor associated with increasing Symptom Severity of incontinence -Diabetes Urinary incontinence Fecal Urgency Hyterectomy Rectal hypersensitivity

5
We evaluated 120 DCR JOURNAL from 2000 to2016 about incontinence treatment

6
Abnormal colonic motility

7
- Obesity

8
Pelvic floor disorder

9
Diabetes Urinary incontinence Fecal Urgency

10
Hysterectomy

11
Rectal hypersensitivity

12
Incontinence Severity Score
1. Wexner incontinence score (0;perfect continence , 20;complete incontinence) 2. Fecal incontinence score by Miller (more than 12; should consider surgical treatment) 3. Vaizy Score 4. FIQL (Fecal Incontinence Quality of Life ) score 5. Reduced quality of life scale (0-10)
 2. Fecal incontinence score by Miller (more than 12; should consider surgical treatment) 3. Vaizy Score 4. FIQL (Fecal Incontinence Quality of Life ) score 5. Reduced quality of life scale (0-10)")
13
Nonoperative management of Incontinence I
Nonoperative management of Incontinence I. Dietary management ; 22% to 54 % of patients can have improvement in fi with formal counseling from a specialist regarding dietary habits, fluid management, bowel routines, and changes to medications II. Pharmacological treatments ; which can slow colonic transit, decrease intestinal fluid secretion, increase absorption, and reduce sphincter relaxation

14
III. Biofeedback treatment IV. Extracorporeal magnetic. stimulation V
III. Biofeedback treatment IV. Extracorporeal magnetic stimulation V. Percutaneous post-tibial stimulation VI.Anal plug VII. Radiofrequency treatment (Secca procedure) VIII. Submucosal collagen, biomaterial injection
 VIII. Submucosal collagen, biomaterial injection.")
15
Pharmacological treatments

16
II. Pharmacological treatments which
II. Pharmacological treatments which Antidiarrheal effect -Loperamide -Diphenoxylate -Atropine -Codeine phosphate (result in decreased intestinal motility, decreased intestinal secretion, and increased absorption) but side effect like nausea, constipation,abdominal pain
 but side effect like nausea, constipation,abdominal pain.")
17
II. Pharmacological treatments which Other effect -Kaopectate -Cholestyramine -Topical Phenylephrine -Hormonal replacement theraphy -Tricyclic antidepressants -Ion exchange resins - Clonidine, (Which is used in diarrheapredominant irritable bowel syndrome reduces rectal sensation and urgency; improving stool consistency and frequency, although the results are not conclusive)
.")
18
Biofeedback treatment

19
-Noninvasive and hence considered a first-line treatment
-Noninvasive and hence considered a first-line treatment option for patients with F.I. -Who not responded to simple dietary modification, medications, and other supportive measures -improve sensation, coordination, and strength - supportive counseling and practical advice regarding diet, bowel habits, and skin care remain important components - 64% to 89% improvement in incontinence episodes

20
화명학운외과 Subjective satisfaction and result of anorectal physiologic study after Biofeedback treatment in incontinence patients according to individual Bowel habit in My Hospital 안녕 하십니까 화명 학운외과 조현언 입니다 제가 오늘 말씀드릴 내용은 변실금환자에서의 대장 증상에 따른 임상소견과 직장항문생리검사의 차이점및 바이오 피드백 치료 후 만족도에 대한 연구 에 대해서 입니다 조현언

21
화명학운외과 일단 전 환자에서의 치료전 후 직장 항문 생리 검사소견wexner score 변화등을 측정 하였고 대장 증상에 따라 임상적인 소그룹으로 분류하여 ;변실금만을 호소한군을그룹1, 변실금과 설사가 동반된 군 을그룹2, 변실금과 변비,설사가 반복 되는 군을그룹3 변실금과 변비가 동반된 군을그룹4로 정하였고 각군에서 직장 항문 내압 소견, 바이오 피드백 치료 후 내압소견, 직장항문억제 반사의 반응정도, 항문 고압력대의 길이측정 하였고 치료 후wexner score 차이, 항문통, 직장통증과 복부팽창,요통증상등의 증상차이 를 확인하였읍니다 Hwamyeong Hakwoon Colorectal Surg Clinic Patients and Method Group 1: Incontinence group Group 2 : Incontinence and Diarrhea group Group 3 : Incontinence and Diarrhea and Constipation group Group 4 : Incontinence and Constipation group Pre-treatment and After treatment anorectal physiology change and Wexner Score change in all patients and bowel habit change after Biofeedback treatment 조현언

22
Result of anorectal physiology after Biofeedback & low current electrical stimulation F/U period ; 12 months (6- 36 months)
")
23
Patient’s satisfaction & wexner score change patient satisfaction wexner score change

24
Group 3 (Incontinence and Diarrhea and Constipation group )
Group 3 (Incontinence and Diarrhea and Constipation group ) ;shows more anal discomfort, more abdominal discomfort and more decreased patient’s satisfaction Group 4 (Incontinence and Constipation group) ;shows more abdominal bloating and discomfort Group 1 (Incontinence group ) ;shows more improved patient’s satisfaction and life of quality after biofeedback treatment
 ;shows more anal discomfort, more abdominal discomfort and more decreased patient’s satisfaction Group 4 (Incontinence and Constipation group) ;shows more abdominal bloating and discomfort Group 1 (Incontinence group ) ;shows more improved patient’s satisfaction and life of quality after biofeedback treatment.")
25
After thease results irritable bowel change group shows more increased anal discomfort , increased abdominal discomfort and decreased patient’s satisfaction after Biofeedback treatment

27
Extracorporeal Magnetic stimulation

29
Magnetic vs Electric Principal of CR-3000 교류강자기장 발생 인체 조직 내 와전류 발생
이런 의구심 없으셨습니까? Magnetic Electric 환자의 통증 유발점이 표피 및 심부에 있다. 표피에서 심부 10cm 이상에 이르기까지 치료 자극한계 체표면 심부까지 치료하고 싶다. 유발전위 활성화 인체 내 왜곡 왜곡 환자는 원인치료 방법은 없을까? 환자만족도 극대화 환자 효과 표면에서의 한시적 효과 병원에서 선택한 치료법을 향상시킬 방법은 없을까? 전기 생리학적인 접근을 통한 폭넓은 치료선택 응용 응용의 한계성 혹시, 환자에게 헤가 되지 않을까? 없음 부작용 피부손상, 통증 유발 가능성 Principal of CR-3000 교류강자기장 발생 인체 조직 내 와전류 발생 와전류에 의한 전기자극 급, 만성 통증 조절 수술 후 통증 조절 Nerve root 자극 2Tesla의 강자기장 발생

30
Magnetic stimulation therphy in my Hospital

31
Journal of the Korean Society of Coloproctology 변실금의 진단과 치료 건국학교 의과학 외과학교실 성 무 경 책임자: 성무경, , 서울시 진구 화양동 4-12 건국학교 병원 외과 EMS (extracorporeal magnetic stimulation) may great success in treatment of anal incontinence 자기장으로 자극을 가하면 신경막의 극화를 초래할 수 있는 자기장이 만 들어 진다는 점에서 천수신경을 체외에서 비침습적으로 자극하는 수단으로 자기장을 활용하기도 한다. 최근에는 회음부에 바로 자기장을 걸어 좀 더 직접적으 로 음부신경을 자극하는 방법을 쓰기도 한다. 음부신 경을 자극하는 것과 천수신경을 자극하는 것은 이론 으로는 그 배경이 다르다. 그러나 바이오피드백의 치료원리를 고려하자면 자기장에 의해서든 아니든 음부신경을 자극하는 것도 효과가 있어야 한다는 점에 서는 EMS도 상당한 성공을 기대 할 수도 있다11

32
The results of Extracorporeal magnetic stimulation in our Hospital After the treatment of magnetic stimulation; - improved result in compliance, rest , squeeze, push, MTV with statistical significance large subjective patient's satisfaction with statistical significance and improved result in defecation habit, defecation interval and time

33
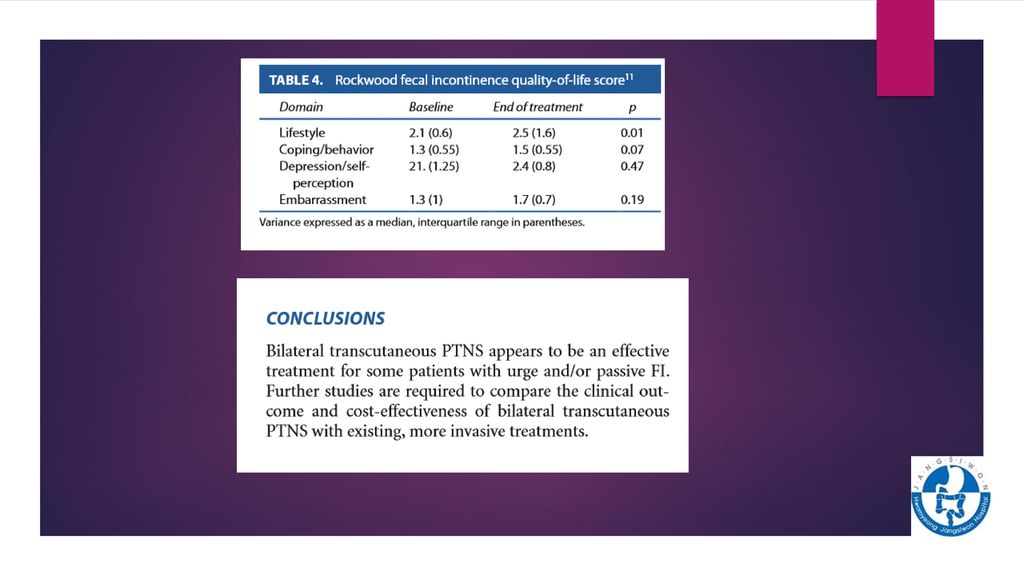
Percutaneous Post-tibial nerve stimulation

37
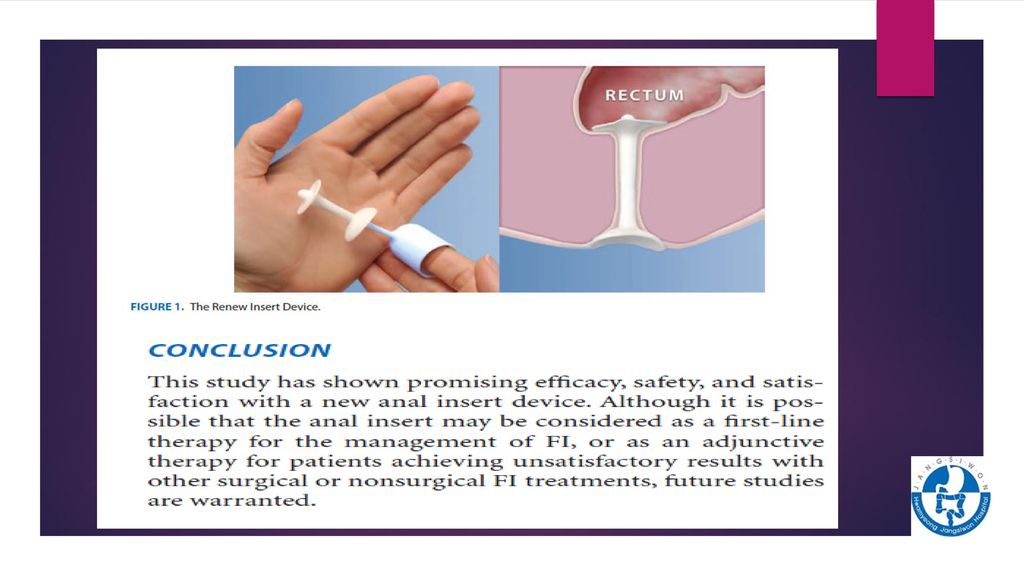
Anal insert device

40
Radiofrequency treatment

41
Injectable collagen treatment

42
Conclusion

43
No fecalith in rectum No leakage

44
In treating incontinence patients not only try to strengthen the sphincter, we should consider his individual bowel habit and pelvic disorder and defecation habit and their cormorbity. So if incontinet patient has defecation disorder , we should treat this defecation disorder first .

45
Thankyou

Similar presentations

 이용 가능한 template.>")





 Congress 참석 및 발표.>")


 주요 내용 소개>")




 1.>")



 비만률순위 : 29 위 (2005 OECD)>")
